Download
1 / 49
570 likes | 2.03k Views
Caries Risk Assessment and Disease Prevention. Thuan Le, DDS, PhD Associate Professor of Clinical Pediatric Dentistry University of California, San Francisco. Objectives. Inspire medical and dental personnel to evaluate oral health status in infants and young children.

E N D
Caries Risk Assessment andDisease Prevention Thuan Le, DDS, PhD Associate Professor of Clinical Pediatric Dentistry University of California, San Francisco
Objectives • Inspire medical and dental personnel to evaluate oral health status in infants and young children. • Be able to assess caries risk and to individualize interventions and recall. • Demonstrate key elements addressed in the knee-to-knee encounter. • Promote the use of fluorides and dental sealants. • Understand and promote the use of early intervention techniques. • Understand motivational interviewing and goal setting. • Promote healthy daily family behaviors for optimal oral health.
You too can see young children and learn to do a Caries Risk Assessment!
Early Childhood Caries (ECC) Any tooth decay, including extractions and fillings from previous decay, in the primary dentition.
Severe Early Childhood Caries (S-ECC) • Distinctive pattern of tooth decay that begins on upper primary teeth. • Rapidly progressing to other teeth as they erupt.
Early Childhood Caries (ECC) in California • California’s children fall well below the nation in oral health. • About 1/3 of preschoolers and almost 70% of children in grades K-3 have experienced tooth decay. Data from the 2006 California Smile Survey
Treatment of ECC • 40-50% of children treated with severe ECC have new decay within 4-12 months. • Restorations alone do not solve the problem. We must treat the infection!
Primary teeth are important! Eating and Nutrition Holding Space Talking Smiling!
White Spot Lesions • The first visible sign of tooth decay is decalcification. • Reversible!
ECC can be prevented. • Interventions with pregnant women and mothers of infants. • Interventions with babies and young children.
Ways to Prevent ECC • Water Fluoridation • Application of Fluoride Varnish • Sealants on primary teeth • Daily brushing with fluoride toothpaste • Dietary changes
Fluoride Varnish • Easily applied topical fluoride treatment • Safe for babies and young children
Dietary Counseling • Limit sugary foods and drinks. • Limit simple carbohydrates like white crackers. • Need to limit both frequency and total sugar intake. • Encourage drinking water and fresh fruit and vegetable snacks.
Limit Total Sugar Intake • Dentistry does not practice in a vacuum. • Increased obesity and diabetes type II among children requires limiting both frequency and total sugar intake.
Weaning • Recommend using a cup at 6 months of age. • Consider weaning at 12-14 months of age. • Don’t let baby sleep with the bottle or walk around with a bottle or sippy cup all day.
Oral Health Assessment andCaries Risk Assessment (CRA) for Babies and Young Children
Supply List • 2X2 gauze • Direct light source • Baby/child toothbrush • Fluoride Varnish • Vinyl/latex gloves • Plastic mirror/tongue blades • Floss
Step 1: Begin assessing risk factors and protective factors • Family history of caries • Bottle use and other dietary habits • Developmental disabilities or special needs • Assess water fluoridation/systemic fluoride supplements • Home care and use of fluoride toothpaste • Dental Home
Building Rapport • Play and talk with child • Use toys or a baby toothbrush for distraction • Use staff to occupy child during the interview
Expect Crying • Bad News: Child is crying. • Good News: You can see the teeth clearly.
Tips for Behavior Management • Focus on the nature of the cry • Use distraction techniques • Tell, show, do Above all, stay calm!
Step 3: Toothbrush Prophy • Remove plaque so you can see teeth clearly • Discuss home care • Reinforce the use of a small smear of fluoride toothpaste
Cleaning the Teeth at Home • Begins when first tooth erupts • Let older children and caregivers practice while you watch
Step 4: Clinical aspects of CRA • Presence of thick plaque • Chalky white spots, brown spots, or obvious dental caries • Tooth defects • Visually inadequate saliva flow
Lift the Lip • Show caregivers any signs of tooth decay • Teach them to “lift the lip” monthly to check for chalky white spots or brown spots
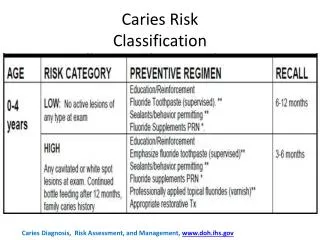
Caries Risk Assessment High risk = Active disease or recent disease activity • White spot lesions • Carious lesions in previous 12 months • Active caries in caregiver Moderate risk = Presence of risk indicator but no active disease • Visible plaque • Frequent carbohydrate exposure • No carious lesions in previous 12 months Low risk = Absence of factors in either category
Fluoride Varnish Procedure • Dry teeth lightly with a gauze square • Open the packet of varnish • Stir with applicator • “Paint” the varnish on the child’s teeth • “Less is More”
Fluoride Varnish Procedure • Begin with lower teeth. Do the outsides of all teeth and then the insides. • Repeat with upper arch. • Develop a pattern that works for you.
Fluoride Varnish Procedure • When in doubt, follow the manufacturer’s instructions
Parent Instructions • Mild yellow or brownish tint that will disappear when the teeth are brushed. • Don’t brush until the next day for optimal benefit.
All done! • Raise the child back into their caregiver’s arms for comforting. • Most children stop crying at this point. • Give them a toothbrush or toy to play with while you talk with the caregiver.
Step 6: Summary and Goal-Setting • Summarize findings, follow-up, and home care. • Discuss risk. • Set goals.
Small Steps • Choose 1-2 key messages • Non-judgmental and friendly • Culturally sensitive • Remain positive!
Multiple Triggers Over Time • Changes in health behavior do not happen overnight. • It often takes many triggers, delivered over a period of time, in combination with a person’s own experiences and values to change health behavior.
Disease Management • Interim Therapeutic Restorations (ITRs) using fluoride-releasing glass ionomer • Silver Diamine Fluoride
Interim Therapeutic Restorations • Minimal cavity preparation, no injections, no drilling • Fluoride releasing glass ionomer • Be sure to inform the family: • That this stops the disease for the time-being • That these fillings will be recharged with fluoride when the child drinks fluoridated water or brushes with fluoride toothpaste • Continued check-ups are important
Silver Diamine Fluoride • Silver’s antibacterial properties; fluoride’s remineralization properties. • Interim Caries Arresting Medicament • CDT Code 1354 • FDA approved for tooth sensitivity; off label use for caries arrest.
Risk-Based Recall Consider: • High risk = 4x/year • Moderate risk = 3x/year • Low risk = 1-2x/year
Reinforce Home Care It’s what families do at home that really counts!
Follow-Up Visits Children who have received infant caries risk assessments often make excellent future dental patients.
6 Steps • Interview • Position the child • Toothbrush Prophy • CRA • Fluoride Varnish Treatment • Summary and Goal Setting