Download
1 / 1
10 likes | 134 Views
No. 132. ESWL for encrusted stents Shockwave lithotripsy for retained encrusted ureteric stents: a review of 27 cases. D.R. Lenaghan , M. Salvatore, J.R. Goad, A.H. Clarke Urology Unit, Department of Surgery, St Vincent’s Hospital, Melbourne. Posters Proudly Supported by: . Introduction

E N D
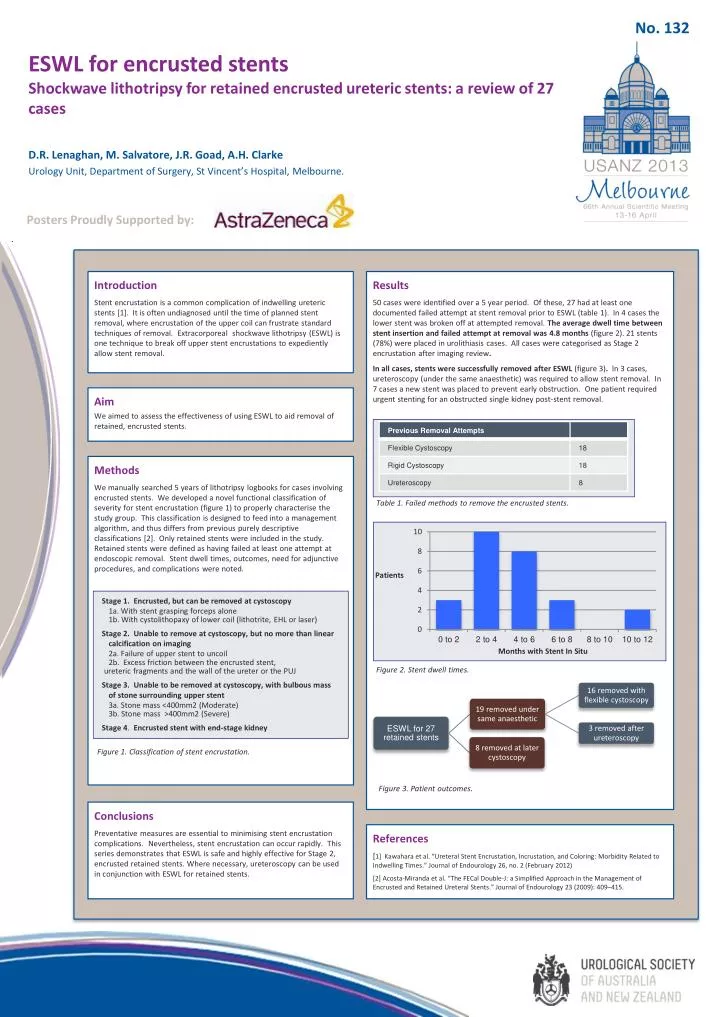
No. 132 ESWL for encrusted stentsShockwave lithotripsy for retained encrusted ureteric stents: a review of 27 cases D.R. Lenaghan, M. Salvatore, J.R. Goad, A.H. Clarke Urology Unit, Department of Surgery, St Vincent’s Hospital, Melbourne. Posters Proudly Supported by: Introduction Stent encrustation is a common complication of indwelling ureteric stents [1]. It is often undiagnosed until the time of planned stent removal, where encrustation of the upper coil can frustrate standard techniques of removal. Extracorporeal shockwave lithotripsy (ESWL) is one technique to break off upper stent encrustations to expediently allow stent removal. Results 50 cases were identified over a 5 year period. Of these, 27 had at least one documented failed attempt at stent removal prior to ESWL (table 1). In 4 cases the lower stent was broken off at attempted removal.The average dwell time between stent insertion and failed attempt at removal was 4.8 months (figure 2). 21 stents (78%) were placed in urolithiasiscases. All cases were categorised as Stage 2 encrustation after imaging review. In all cases, stents were successfully removed after ESWL (figure 3). ln 3 cases, ureteroscopy (under the same anaesthetic) was required to allow stent removal. In 7 cases a new stent was placed to prevent early obstruction. One patient required urgent stenting for an obstructed single kidney post-stent removal. Aim We aimed to assess the effectiveness of using ESWL to aid removal of retained, encrusted stents. Methods We manually searched 5 years of lithotripsy logbooks for cases involving encrusted stents. We developed a novel functional classification of severity for stent encrustation (figure 1) to properly characterise the study group. This classification is designed to feed into a management algorithm, and thus differs from previous purely descriptive classifications [2]. Only retained stents were included in the study. Retained stents were defined as having failed at least one attempt at endoscopic removal. Stent dwell times, outcomes, need for adjunctive procedures, and complications were noted. Table 1. Failedmethodstoremovetheencrustedstents. Patients Stage 1. Encrusted, but can be removed at cystoscopy 1a. With stent grasping forceps alone 1b. With cystolithopaxy of lower coil (lithotrite, EHL or laser) Stage 2. Unable to remove at cystoscopy, but no more than linear calcification on imaging 2a. Failure of upper stent to uncoil 2b. Excess friction between the encrusted stent, ureteric fragments and the wall of the ureter or the PUJ Stage 3. Unable to be removed at cystoscopy, with bulbous mass of stone surrounding upper stent 3a. Stone mass <400mm2 (Moderate) 3b. Stone mass >400mm2 (Severe) Stage 4. Encrusted stent with end-stage kidney MonthswithStent In Situ Figure 2. Stentdwell times. Figure 1. Classification of stentencrustation. Figure3. Patientoutcomes. Conclusions Preventative measures are essential to minimising stent encrustation complications. Nevertheless, stent encrustation can occur rapidly. This series demonstrates that ESWL is safe and highly effective for Stage 2, encrusted retained stents. Where necessary, ureteroscopy can be used in conjunction with ESWL for retained stents. References [1] Kawahara et al. “Ureteral Stent Encrustation, Incrustation, and Coloring: Morbidity Related to Indwelling Times.” Journal of Endourology 26, no. 2 (February 2012) [2] Acosta-Miranda et al. “The FECal Double-J: a Simplified Approach in the Management of Encrusted and Retained Ureteral Stents.” Journal of Endourology23(2009): 409–415.






