Download
1 / 4
40 likes | 149 Views
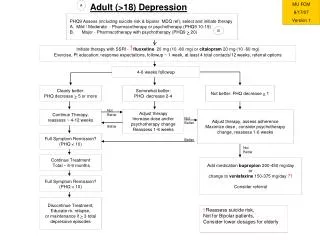
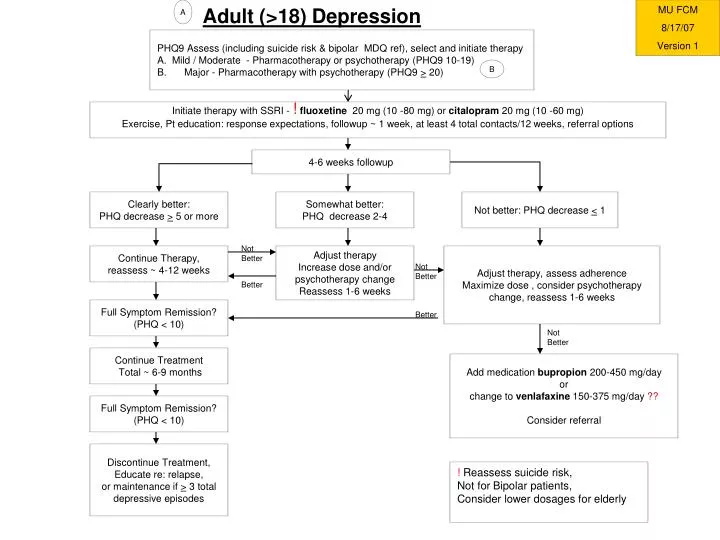
Adult (>18) Depression. A. MU FCM 8/17/07 Version 1. PHQ9 Assess (including suicide risk & bipolar MDQ ref), select and initiate therapy A. Mild / Moderate - Pharmacotherapy or psychotherapy (PHQ9 10-19) Major - Pharmacotherapy with psychotherapy (PHQ9 > 20). B.

E N D
Adult (>18) Depression A MU FCM 8/17/07 Version 1 • PHQ9 Assess (including suicide risk & bipolar MDQ ref), select and initiate therapy • A. Mild / Moderate - Pharmacotherapy or psychotherapy (PHQ9 10-19) • Major - Pharmacotherapy with psychotherapy (PHQ9 > 20) B Initiate therapy with SSRI - !fluoxetine 20 mg (10 -80 mg) or citalopram 20 mg (10 -60 mg) Exercise, Pt education: response expectations, followup ~ 1 week, at least 4 total contacts/12 weeks, referral options 4-6 weeks followup Clearly better: PHQ decrease > 5 or more Somewhat better: PHQ decrease 2-4 Not better: PHQ decrease < 1 Not Better Continue Therapy, reassess ~ 4-12 weeks Adjust therapy Increase dose and/or psychotherapy change Reassess 1-6 weeks Adjust therapy, assess adherence Maximize dose , consider psychotherapy change, reassess 1-6 weeks Not Better Better Full Symptom Remission? (PHQ < 10) Better Not Better Continue Treatment Total ~ 6-9 months Add medication bupropion 200-450 mg/day or change to venlafaxine 150-375 mg/day ?? Consider referral Full Symptom Remission? (PHQ < 10) Discontinue Treatment, Educate re: relapse, or maintenance if > 3 total depressive episodes ! Reassess suicide risk, Not for Bipolar patients, Consider lower dosages for elderly
MU FCM 8/17/07 Version 1 A Osteoarthritis Non- Pharmacologic methods: Self management, Exercise or Physical therapy, Weight loss Pain & functional assessment each visit Acetaminophen up to 1 gm po QID ! Knee - Consider Orthotics (lateral wedge [podiatry], taping [PT]), consider trial of glucosamine 1500 mg/d Hands – splint for thumbs Consider topical Capsaicin – 0.025 % cream to skin TID/QID Knee - If knee joint effusion present, consider aspiration and intra-articular corticosteroids 40 mg Triamcinolone NSAID: Naproxen 250 - 500 mg po BID or Naproxen Sodium 220-550 mg po BID or Salsalate 1500 mg po BID If GI risk factors (Age > 65, Hx PUD/GI Bleed, Steroid, ASA, or warfarin use, smoker, EtOH use) may add omeprazole 20 mg po daily If renal ds, no response, or age > 65, consider Tramadol 50 mg daily to QID, or Opiates: Acetaminophen/codeine 30 mg QID or Acetaminophen/hydrocodone 5 mg 1-2 tabs QID If no response, consider change of NSAID (Diclofenac 50 mg BID) or EC Aspirin 650 mg TID or COX 2 inhibitor (Celecoxib 200 mg daily) Knee – consider intra-articular Synvisc 2 ml weekly X 3 weeks Specialist referral ! –Caution with long term use/liver ds
COPD (FEV1/FVC < 70%)Smoking Cessation, Education (activities, MDI, SX, breathing), Immunizations Ref: ACP and Gold