Download
1 / 22
260 likes | 764 Views
Hyaline Membrane Disease. Li wei-zhong. Introduction. HMD, frequently referred to as neonatal respiratory distress syndrome (NRDS), occurs primarily in premature infant. There is rapid or labored breathing, beginning at or immediately after birth.

E N D
Hyaline Membrane Disease Li wei-zhong
Introduction • HMD, frequently referred to as neonatal respiratory distress syndrome (NRDS), occurs primarily in premature infant. • There is rapid or labored breathing, beginning at or immediately after birth. • Surfactant deficiency is the primary cause of HMD.
Epidemiology • HMD occurs primarily in Premature infant • Infants less than 28 wk of GA: 60-80% • Infants between 28 and 32 wk: 60% • Infants between 32 and 36wk of GA: 15-30% • Infants beyond 37 wk of GA: 5%
Epidemiology • The incidence of HMD is highest among premature male or white infants. • The incidence is higher for cesarean section without labor than vaginal delivery. • HMD is more common in gestational diabetes and in insulin-dependent mother. • Second-born twin is at greater risk.
Etiology • Surfactant Deficiency • Prematurity predisposes • Cesarean section • Male > female • White > nonwhite • Second- born twin
Etiology • Maternal diabetes • Maternal hemorrhage • Maternal stress • Intrauterine growth retardation • Prolonged rupture of membranes (>16 hr) • Asphyxia
Etiology • Hypoxemia • Pulmonary Ischemia • Hypovolemia and Hypotension • Cold Stress • High Oxygen concentration
Pathophysiology • Surfactant deficiency increases surface tension in Alveolus • Surfactant decreases surface tension in the alveolus during expiration, allowing the alveolus to remain partly expanded and in that way maintaining a functional residual capacity.
Pathophysiology • The surface tension in the alveolus results in poor lung compliance and atelectasis. • decreased tidal volumes • increased physiologic dead space • Poor lung distensibility • Poor alveolar stability
Pathophysiology • increased work of breathing • perfused but not ventilated alveoli • Ventilated but not perfused alveoli • Respiratory failure
Pathophysiology • The combination of hypercarbia, hypoxia and acidosis produces pulmonary arterial vasoconstriction with increased right-to-left shunting through the foramen ovale and ductus arteriosus and within the lung itself. • Reduced effective pulmonary blood flow
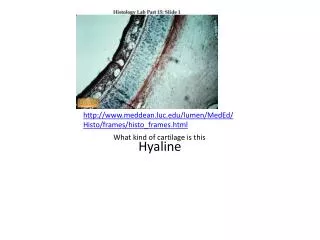
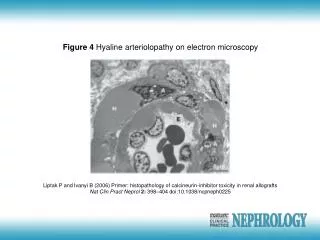
Pathology • Lung extensive atelectasis • Injury to epithelial calls • Lung congestion and edema • Lung hemorrhage • Hyaline membranes contains fibrin and cellular products
Clinical Findings • Onset near the time of birth or within 4-6 hr after birth • Rapid, shallow respirations ≥ 60/ min • Intercostal and subcostal retractions and progressive respiratory distress • Expiratory grunt • Cyanosis or pallor
Clinical Findings • Hypothermia • hypotension • Fine inspiratory rales • Pulmonary or intraventricular hemorrhage • Course to death or improvement 3-5d
Clinical Findings • Laboratory diagnosis • Arterial blood gases • Hypoxemia • Hypercapnia • Mixed respiratory-metabolic Acidemia
Clinical Findings • Lecithin/sphingomyelin ratio (L/S)<2:1 • Low phosphatidylglycerol(PG) • Low saturated phosphatidylcholine (PC) • Low surfactant protein A/saturated PC (SP-A/SPC) ratio
Clinical Findings • Chest x-ray • Typical pattern at 24 hr after birth • Ground-glass appearance • Air bronchograms • Doming of diaphragm and underexpansion (white out)
Diagnosis • Tachypnea, cyanosios, and expiratory grunting • Poor air movement despite increased work of breathing • Blood gases, pH values, and other laboratory finding • Chest x-ray showing hypoexpansion and air bronchograms
Differential Diagnosis • Wet lung of the newborn (Transient dyspnea) • Amniotic fluid and meconium aspiration syndrome • Group B streptococcal pneumonia • Diaphragmatic hernia
Treatment • The basic defect requiring treatment is inadequate pulmonary exchange of oxygen and carbon dioxide. • Metabolic acidosis and circulatory insufficiency are secondary manifes-tations.
Treatment • Supportive care of LBW infant • Surfactant replacement therapy • Oxygen therapy • Continuous positive airway pressure (CPAP) • Assisted mechanical ventilation • Blood pressure support • Alkali therapy
Prevention • Prenatal glucocorticoids for >24 hr • Prophylactic administration of exogenous surfactant at birth