Download
1 / 1

E N D
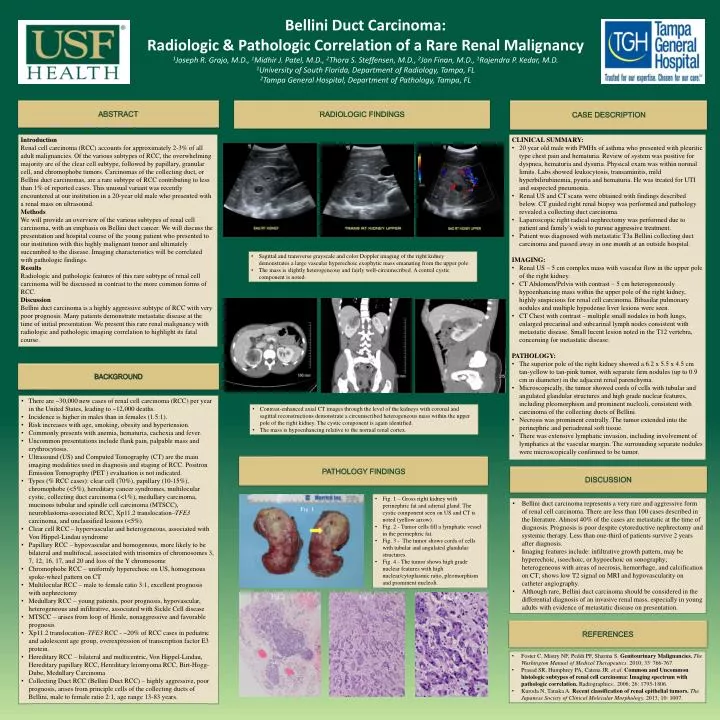
Bellini Duct Carcinoma: Radiologic & Pathologic Correlation of a Rare Renal Malignancy1Joseph R. Grajo, M.D., 1Midhir J. Patel, M.D., 2Thora S. Steffensen, M.D., 2Jon Finan, M.D.,1Rajendra P. Kedar, M.D.1University of South Florida, Department of Radiology, Tampa, FL2Tampa General Hospital, Department of Pathology, Tampa, FL CASE DESCRIPTION ABSTRACT RADIOLOGIC FINDINGS Introduction Renal cell carcinoma (RCC) accounts for approximately 2-3% of all adult malignancies. Of the various subtypes of RCC, the overwhelming majority are of the clear cell subtype, followed by papillary, granular cell, and chromophobe tumors. Carcinomas of the collecting duct, or Bellini duct carcinomas, are a rare subtype of RCC contributing to less than 1% of reported cases. This unusual variant was recently encountered at our institution in a 20-year old male who presented with a renal mass on ultrasound. Methods We will provide an overview of the various subtypes of renal cell carcinoma, with an emphasis on Bellini duct cancer. We will discuss the presentation and hospital course of the young patient who presented to our institution with this highly malignant tumor and ultimately succumbed to the disease. Imaging characteristics will be correlated with pathologic findings. Results Radiologic and pathologic features of this rare subtype of renal cell carcinoma will be discussed in contrast to the more common forms of RCC. Discussion Bellini duct carcinoma is a highly aggressive subtype of RCC with very poor prognosis. Many patients demonstrate metastatic disease at the time of initial presentation. We present this rare renal malignancy with radiologic and pathologic imaging correlation to highlight its fatal course. • CLINICAL SUMMARY: • 20 year old male with PMHx of asthma who presented with pleuritic type chest pain and hematuria. Review of system was positive for dyspnea, hematuria and dysuria. Physical exam was within normal limits. Labs showed leukocytosis, transaminitis, mild hyperbilirubinemia, pyuria and hematuria. He was treated for UTI and suspected pneumonia. • Renal US and CT scans were obtained with findings describedbelow. CT guided right renal biopsy was performed and pathology revealed a collecting duct carcinoma. • Laparoscopic right radical nephrectomy was performed due to patient and family’s wish to pursue aggressive treatment. • Patient was diagnosed with metastatic T3a Bellini collecting duct carcinoma and passed away in one month at an outside hospital. • IMAGING: • Renal US – 5 cm complex mass with vascular flow in the upper pole of the right kidney. • CT Abdomen/Pelvis with contrast – 5 cm heterogeneously hypoenhancingmass within the upper pole of the right kidney, highly suspicious for renal cell carcinoma. Bibasilar pulmonary nodules and multiple hypodense liver lesionswere seen. • CT Chest with contrast – multiple small nodules in both lungs, enlarged precarinal and subcarinal lymph nodes consistent with metastatic disease. Small lucent lesion noted in the T12 vertebra, concerning for metastatic disease. • PATHOLOGY: • The superior pole of the right kidney showed a 6.2 x 5.5 x 4.5 cm tan-yellow to tan-pink tumor, with separate firm nodules (up to 0.9 cm in diameter) in the adjacent renal parenchyma. • Microscopically, the tumor showed cords of cells with tubular and angulated glandular structures and high grade nuclear features, including pleomorphism and prominent nucleoli, consistent with carcinoma of the collecting ducts of Bellini. • Necrosis was prominent centrally. The tumor extended into the perinephric and periadrenalsoft tissue. • There was extensive lymphatic invasion, including involvement of lymphatics at the vascular margin. The surrounding separate nodules were microscopically confirmed to be tumor. • Sagittal and transverse grayscale and color Doppler imaging of the right kidney demonstrates a large vascular hyperechoic exophytic mass emanating from the upper pole. • The mass is slightly heterogeneous and fairly well-circumscribed. A central cystic component is noted. BACKGROUND • There are ~30,000 new cases of renal cell carcinoma (RCC) per year in the United States, leading to ~12,000 deaths. • Incidence is higher in males than in females (1.5:1). • Risk increases with age, smoking, obesity and hypertension. • Commonly presents with anemia, hematuria, cachexia and fever. • Uncommon presentations include flank pain, palpable mass and erythrocytosis. • Ultrasound (US) and Computed Tomography (CT) are the main imaging modalities used in diagnosis and staging of RCC. Positron Emission Tomography (PET ) evaluation is not indicated. • Types (% RCC cases): clear cell (70%), papillary (10-15%), chromophobe(<5%), hereditary cancer syndromes, multilocularcystic, collecting duct carcinoma (<1%), medullary carcinoma, mucinous tubular and spindle cell carcinoma (MTSCC), neuroblastoma-associated RCC, Xp11.2 translocation–TFE3 carcinoma, and unclassified lesions (<5%). • Clear cell RCC – hypervascular and heterogeneous, associated with Von Hippel-Lindausyndrome • Papillary RCC – hypovascular and homogenous, more likely to be bilateral and multifocal, associated with trisomies of chromosomes 3, 7, 12, 16, 17, and 20 and loss of the Y chromosome • Chromophobe RCC – uniformly hyperechoic on US, homogenous spoke-wheel pattern on CT • Multilocular RCC – male to female ratio 3:1, excellent prognosis with nephrectomy • MedullaryRCC – young patients, poor prognosis, hypovascular, heterogeneous and infiltrative, associated with Sickle Cell disease • MTSCC – arises from loop of Henle, nonaggressive and favorable prognosis • Xp11.2 translocation–TFE3 RCC - ~20% of RCC cases in pediatric and adolescent age group, overexpression of transcription factor E3 protein. • Hereditary RCC – bilateral and multicentric, Von Hippel-Lindau, Hereditary papillary RCC, Hereditary leiomyoma RCC, Birt-Hogg-Dube, Medullary Carcinoma • Collecting Duct RCC (Bellini Duct RCC) – highly aggressive, poor prognosis, arises from principle cells of the collecting ducts of Bellini, male to female ratio 2:1, age range 13-83 years. • Contrast-enhanced axial CT images through the level of the kidneys with coronal and sagittal reconstructions demonstrate a circumscribed heterogeneous mass within the upper pole of the right kidney. The cystic component is again identified. • The mass is hypoenhancing relative to the normal renal cortex. PATHOLOGY FINDINGS DISCUSSION • Fig. 1 – Gross right kidney with perinephric fat and adrenal gland. The cystic component seen on US and CT is noted (yellow arrow). • Fig. 2 - Tumor cells fill a lymphatic vessel in the perinephric fat. • Fig. 3 - The tumor shows cords of cells with tubular and angulated glandular structures. • Fig. 4 - The tumor shows high grade nuclear features with high nuclear/cytoplasmic ratio, pleomorphism and prominent nucleoli. • Bellini duct carcinoma represents a very rare and aggressive form of renal cell carcinoma. There are less than 100 cases described in the literature. Almost 40% of the cases are metastatic at the time of diagnosis. Prognosis is poor despite cytoreductive nephrectomy and systemic therapy. Less than one-third of patients survive 2 years after diagnosis. • Imaging features include: infiltrative growth pattern, may be hyperechoic, isoechoic, or hypoechoic on sonography; heterogeneous with areas of necrosis, hemorrhage, and calcification on CT; shows low T2 signal on MRI and hypovascularityon catheter angiography. • Although rare, Bellini duct carcinoma should be considered in the differential diagnosis of an invasive renal mass, especially in young adults with evidence of metastatic disease on presentation. Fig. 1 Fig. 2 Fig. 3 Fig. 4 REFERENCES • Foster C, Mistry NF, Peddi PF, Sharma S. Genitourinary Malignancies. The Washington Manual of Medical Therapeutics. 2010; 33: 766-767. • Prasad SR, Humphrey PA, Catena JR. et al. Common and Uncommon histologic subtypes of renal cell carcinoma: Imaging spectrum with pathologic correlation. Radiographics.. 2006; 26: 1795-1806. • Kuroda N, Tanaka A. Recent classification of renal epithelial tumors. The Japanese Society of Clinical Molecular Morphology. 2013; 10: 1007.






