Download
1 / 53
560 likes | 788 Views
Tropical diseases and the Gastrointestinal system. Ahmed Laving ESPGHAN Post Graduate Course 2013. Case 1. 3 yr old girl from Western Kenya c/o diarrhoea for 6 wks Stools x6-10/day (x3 at night), mucoid , occasionally bloody, foul smelling, tenesmus

E N D
Tropical diseases and the Gastrointestinal system Ahmed Laving ESPGHAN Post Graduate Course 2013
Case 1 • 3 yr old girl from Western Kenya • c/o diarrhoea for 6 wks • Stools x6-10/day (x3 at night), mucoid, occasionally bloody, foul smelling, tenesmus • Intermittent fevers, mouth sores, rashes, joint pains but no joint swelling • No h/o contact with PTB • Weight gain appropriate
Case 1 (..2) • PMH: first episode of mucoid stools at 6 months of age; intermittent symptoms • Repeated courses of antibiotics, metronidazole • Positive family h/o atopy and had multiple food allergies (milk, wheat, bananas) • Had been on elemental milk with initial response but with periodic flares • Diagnosis?
Case 1: (..3) • Fair GC, P°, J°, afebrile, not dehydrated • Wt: 14 kg, Ht: 91 cm, MUAC 17.5 cm • Aphthuous mouth sores, healed skin lesions, perianalerythema, no anal tags or fissures • Hb: 10.1, MCV 60, ESR 28, Eos: 6%, Albumin 40 • Stool: occult blood +ve, few pus cells + RBC’s, Campylobacter sensitive to azithromicin • Endoscopy: oesophagitis, gastritis, pancolitis (non-specific, normal eosinophil counts)
Case 1: Diagnosis? • Infectious enteropathy (Campylobacter) • Allergic enteropathy • ?Inflammatory Bowel Disease (IBD)
Case 1: Final diagnosis • Management: • Azithromicin: no response, repeat stool c/s -ve • Dietary elimination of dairy, wheat products • Prednisone (tapered off), sulfasalazine (?IBD) • Recurring episodes of fever, bloody, mucoid stools (compliant to dietary elimination, drugs) • Inadvertent finding: Father of child on ARV’s! • Elisa for HIV: positive • Child started on ARV’s with resolution of symptoms • Final Diagnosis: HIV enteropathy
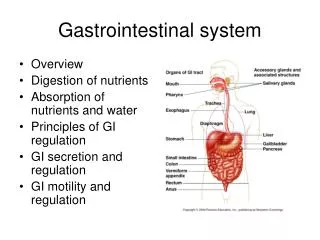
Tropical diseases and GIT • HIV and the GIT • Malnutrition associated enteropathy • Tropical sprue • Sickle cell hepatopathy • Amoebic liver abscess • Schistosomal liver disease
HIV and the GIT • Uncommon if CD4 >200 • Oropharynx: Thrush, hairy leukoplakia, ulcers • Oesophagus: Candida, HSV, CMV • Small/large intestines: chronic diarrhoea • Bacterial: Salmonella, Shigella, Campylobacter, TB • Fungal: Histoplasma, Coccidiomycosis • Protozoa: Cryptosporidia, Microsporidia, Isospora • Others: CMV colitis, C. difficile, bacterial overgrowth • Rectum: Kaposi’s Sarcoma, HSV, condylomata, Non-Hodgkins lymphoma
Oesophagus • Oesophagitis-Burning retrosternal pain, odynophagia. • Candida • HSV-Multiple small ulcers • CMV-Solitary large ulcer
HIV: Small/Large Intestine disease • Usual presentation: diarrhoea with colicky abdominal pain ± fever and weight loss • Bacterial causes are common • Salmonella • 20x more likely to get non-typhoid salmonella • Severe disease with relapses • Long term ciprofloxacin may be necessary • Shigella, Campylobacter, Mycobacteria (MAC)
ProtozoalInfections • Usually manifest with fever, watery diarrhea, nausea, vomiting, abdominal pain, dehydration, weight loss • Cryptosporidia 1% per yr in those with CD4< 300 50% respond to Nitazoxanide (long courses) • Microsporidia May require stool EM, intestinal aspirate or biopsy Extra-intestinal features: eye, muscle and liver • Isospora Peripheral eosinophilia Septrin, Ciprofloxacin • Giardiasis: chronic diarrhoea with malabsorption
Other Causes of Diarrhoea • CMV colitis • Nonbloody diarrhoea • Endoscopy: multiple ulcerative lesions • Biopsy: intranuclear inclusion bodies • May induce vasculitis in the colon/distal small bowel resulting in GI bleeding. • Clostridium difficile- drugs • Neoplasticdisease: Kaposis/NHL • Small bowel bacterial overgrowth
Bacterial Overgrowth • A syndrome of diarrhoea with attendant malabsorption • Uncommon in immuno-competent individuals • Predisposing factors: Impaired intestinal immunity, motility and gastric hypoacidity • Rx: broad spectrum antibiotics • Duration of Rx unknown
HIV Enteropathy • Syndrome of non-infective diarrhoea • Possible pathogenetic mechanisms: • direct infection of the enterocyte by HIV • infection of the lymphoid tissue of the GIT with dysregulation of local cytokine production • Secondary damage due to opportunistic infections • Prevalence and impact of diarrhea on health-related quality of life in HIV-infected patients in the era of highly active antiretroviral therapy. • Siddiqui U, Bini EJ, Chandarana K, Leong J, Ramsetty S, Schiliro D, Poles M J ClinGastroenterol. 2007;41(5):484. • **A prospective study of diarrhea and HIV-1 infection among 429 Zairian infants.Thea DM, St Louis ME, Atido U, Kanjinga K, Kembo B • , Matondo M, Tshiamala T, Kamenga C, Davachi F, Brown C N Engl J Med. 1993;329(23):1696
HIV Enteropathy (2) • Diagnostic workup: • Stools: mcs, AAFB staining (cryptosporidia, cyclospora), trichrome staining (microspora) • Blood cultures: if suspect disseminated disease • Endoscopy: colitis, multiple ulcers, lymphoma • CT abdomen • >50% of diarrhoeal illnesses in HIV-infected individuals no identifiable pathogen *Physiological effects of HIV infection on human intestinal epithelial cells: an in vitro model for HIV enteropathy.Asmuth DM, Hammer SM, Wanke CA AIDS. 1994;8(2):205 **Diagnostic strategies in HIV-infected patients with diarrhea. Mayer HB, Wanke CA AIDS. 1994;8(12):1639.
HIV Enteropathy: Treatment • Antiretroviral therapy: early initiation with reduced incidence of diarrhoea • Empiric antimicrobial use: nitazoxanide, metronidazole, ciprofloxacin (2-3 weeks) • Specific Rx: antivirals, pyrimethamine • ?Antimotility agents, ?probiotics • Zinc supplementation not shown to alter duration or severity in adults *Malabsorption and wasting in AIDS patients with microsporidia and pathogen-negative diarrhea.Lambl BB, Federman M, Pleskow D, Wanke CA AIDS. 1996;10(7):739. **Randomized controlled trial of zinc supplementation for persistent diarrhea in adults with HIV-1 infection. Cárcamo C, Hooton T, Weiss NS, Gilman R, Wener MH, Chavez V, Meneses R, Echevarria J, Vidal M, Holmes K J Acquir Immune DeficSyndr. 2006;43(2):197
Malnutrition Associated Enteropathy(Environmental Enteropathy)
Malnutrition and Diarrhoea Convalescent period not enough to catch up nutrients Reduced food input Reduced immunity Malnutrition Diarrhoeal disease Increased nutritional demand
Infant Diets • Review of 42 infant feeding studies published 1996-2006: (Dewey and Adu-Afarwuah, 2008) • Children who received interventions gained •0-760 g more weight (0.0 – 0.76 WAZ) •0 – 1.7 cm taller (0.0 – 0.64 LAZ) • The very best of these interventions produced a 0.7 Z-score improvement • BUT, the average growth deficit of African and Asian children is –2.0 Z-score • At best, diet solved 1/3 of the problem
Environmental Enteropathy (EE) • A major cause of child undernutrition may be a subclinical inflammation of small intestine • EE: Chronic inflammation of the gut, characterised by: • Villous flattening • Modest malabsorption • Inflammatory cell infiltrate • Increased permeability • Bacterial overgrowth
Environmentalenteropathy (2) • Starved infants pass frequent green liquid stools of small volume (less than 10 grams) • Pathogenesis • Impaired development and function of the immune system, therefore increase in enteric infection • generalized increase in inflammatory mediators • impaired tissue repair mechanisms • Specific nutrient deficiencies, such as vitamin A and zinc deficiencies
EE: Management • Inpatient or outpatient management of malnutrition • Multivitamin (and zinc) supplementation • Empiric use of antibiotics • Improve hygiene and sanitation • Role of anti-inflammatory agents (?mesalamine)
Tropical sprue • A syndrome of acute or chronic diarrhoea, weight loss and malabsorption. • Occurs in the tropics and subtropics • Aetiology unknown, but intestinal microbial infection may cause the initial insult • Coliform bacteria (E.coli, Klebsiella, Enterobacter) usual organisms isolated
Tropical sprue (2) • Pathogenesis: • Infection results in enterocyte injury, intestinal stasis and possible bacterial overgrowth • Results in malabsorption with deficiencies of Iron, Folate, B12 • Affects people who live in areas with sprue as well as travellers who stay for > 1 month
Tropical sprue (3) • CBC: megaloblasticanaemia, Iron deficiency • Diagnosis: endoscopy • Tropical sprue involves the entire small bowel • Gross findings at endoscopy include flattening of duodenal folds and "scalloping” • Histology: shortened, blunted villi and elongated crypts with increased inflammatory cells • Must rule out other causes of diarrhoea, especially infective
Tropical Sprue: Management • Antibiotics for 3-6 months • Folate, Vitamin B12, Iron supplements • No role for antibiotic prophylaxis to prevent sprue
Giardiasis (2) • clinical manifestations*: • 50 %: asymptomatic and clear the infection • 5 to 15% asymptomatic shed cysts • 35 to 45% of individuals have symptomatic infection: • Acute disease • Chronic disease • Diagnosis: • Stool microscopy * 2012 UpToDate ,Release: 20.9 - C20.24
Epidemiology • Amoebic liver abscesses (ALA) most common extraintestinal site of infection of E histolytica • occur in fewer than 1%infections • ALA is 10 times more common in adult males than females while colonic infection is identical in males and females
Clinical Presentation: • Subacute fever • Right upper quadrant pain • May have protracted diarrhoea, abdominal pain, with weight loss • Up to 50% patients have evidence of colonic disease • Jaundice – uncommon, presence suggests multiple abscesses/severe disease
Investigations: laboratory • Hemogram: • Increased WBC (≤75% cases), no eosinophillia • Liver Enzymes: • Increased liver transaminases (≤ 75% cases) • Stool microscopy: • Neither sensitive nor specific • Serology: • Up to 90% positive after 1 week of symptoms
Investigations: Imaging Ultrasonography 90% sensitivity – user dependant CT scan Usually solitary involve right lobe of the liver
Treatment: • Metronidazole 35-50mg/kg/d for 7-10 days • Luminal amoebicide to control intestinal cysts (diloxanidefuroate, iodoquinol) – present in ≤ 60% patients following treatment of ALA • Cure rates of up to 90% with metronidazole • No advantage of percutaneous drainage of an uncomplicated abscess
Schistosomal liver disease (2) • One of the most common causes of noncirrhotic portal hypertension in the world • S. Japonicum, S. Mansoni and S. Hematobium • Schistosomal eggs induce periportal fibrosis, by inducing chronic inflammation once they are trapped in terminal portal veins • Clinical features: of portal hypertension, and of growth retardation Hepatic schistosomiasis. Dunn MA, Kamel R Hepatology. 1981;1(6):653. 2012 UpToDate ,Release: 20.9 - C20.24
Schistosomal liver disease (3) • Underlying hepatic function remains preserved • Diagnosis • detection of schistosomal ova in the stool • biopsies of the rectal mucosa or the liver • immunologic assays • Treatment • Praziquantel (20mg/kg/dose TID for 1 day) in acute stage • Treating complications of portal hypertension • Immunopathogenesis of schistosomiasis. Wynn TA, Thompson RW, Cheever AW, Mentink-Kane MM Immunol Rev. 2004;201:156. • Praziquantel side effects and efficacy related to Schistosomamansoni egg loads and morbidity in primary school children • in north-east Ethiopia. Berhe N, Gundersen SG, Abebe F, Birrie H, Medhin G, GemetchuTActa Trop. 1999;72(1):53.
Sickle cell hepatopathy (2) • Clinical syndrome characterized by marked hyperbilirubinaemia, not explained by severe haemolysis, viral hepatitis, hepatic sequestration or extra-hepatic obstruction • Classified into two categories: • a milder self-limited form without severe hepatic dysfunction • a severe form characterized by fulminant liver failure with coagulopathy and encephalopathy Pediatr Blood Cancer 2005;45:184-190
Sickle cell hepatopathy (3) Complications • Due to disease itself: • Sickle cell vasculopathy • Pigment gall stones due to chronic haemolysis • Acute hepatic crises • Hepatic sequestration • Due to treatment : • Chronic blood transfusions: iron overload 2012 UpToDate ,Release: 20.9 - C20.24
Sickle cell hepatopathy (4) • Evaluation recommended in any child with jaundice > 13 mg/dl ( >220 μmol/L) without evidence of acute severe haemolysis • complete blood count • coagulopathy panel • viral hepatitis serology • appropriate imaging (abdominal ultrasound or CT scan) to r/o biliary sludge, stones • Renal function (hepato-renal syndrome)
Sickle cell hepatopathy: Treatment • Non-severe disease: • Simple transfusion • Supportive management for sickle cell disease • Severe Disease: • Exchange transfusion: only effective therapy • Supportive treatment • ? Role of hydroxyurea, ursodeoxycholic acid
Case 2 • 14 year old boy with blood per rectum for 6 months • Frank blood, tablespoon full, not associated with pain • No h/o constipation • No h/o bleeding disorder • Boarding school in Eastern Kenya
Case 2 • Examination: NAD! • Diagnosis? • Management? • Colonoscopy: 1 pedunculated polyp at 25cm, removed • Histology: juvenile retention polyp with multiple eggs of Schistosoma!
Case 3 • 4 yr old Kenyan Asian girl, known “asthmatic” child with recurrent chest infections since birth • c/o: loose stools since late infancy (1st mention!) • X1-2/day, oily, bulky stools, foul smelling, worse with fatty foods, not readily flushable • No abdominal pain, vomiting, jaundice, pruritus • Poor weight gain, normal milestones • Strong family h/o atopy, consanguineous parents
Case 3: cont’d • Fair GC, P°, J°, afebrile, no pedal oedema • Malnourished: Wt: 9.5 kg (<3SD), Ht: 90 cm (<3SD) • ENT: rhinorrhoea, Chest clear • Abdomen: soft , not distended, non tender, no masses/organomegally • Stool: fecal fat present, pH/reducing substances not done, occult blood negative • Hb: 10.3, MCV: 70, WBC: 8.5, Platelet 195, Albumin: 28