Download
1 / 20
300 likes | 732 Views
PHM142 Fall 2012 Coordinator: Dr. Jeffrey Henderson Instructor: Dr. David Hampson. Cerebral Ischemia. Brandon Wu, Joyce ( Shuo ) Wang, Jonathan (Chun Fung) Lee, Alexis ( Gaoqian ) Yan. What is it?. Insufficient blood flow to the brain

E N D
PHM142 Fall 2012 Coordinator: Dr. Jeffrey Henderson Instructor: Dr. David Hampson Cerebral Ischemia Brandon Wu, Joyce (Shuo) Wang, Jonathan (Chun Fung) Lee, Alexis (Gaoqian) Yan
What is it? • Insufficient blood flow to the brain • Inability of brain tissues to meet its metabolic needs • Leads to brain hypoxia • Prolonged cerebral ischemia can lead to cerebral infarction http://www.pharmaceutical-int.com/suppliers/venous-thromboembolism-risk.html
Focal Ischemia • Blockage of a cerebral vessel • Brain ischemia forms at that specific region • Characterized by a dense, central core of ischemic tissue, and a margin of less dense tissues http://www.elements4health.com/scientists-identify-signal-that-triggers-brain-damage-during-strokes.html
Global Ischemia • Decrease in total brain circulation • Most common cause is cardiac arrest • Reperfusion occurs if blood flow to the brain is restored (transient global ischemia) • Most brain tissues can recover after global ischemia
Symptoms • Blindness in one eye • Weakness in arms or legs • Weakness in one side of the body • Dizziness • Double vision • Vertigo • Slurred speech • Loss of coordination • symptoms can become permanent with cerebral infarction
Causes • Narrowing of arteries, usually caused by atherosclerosis (embolus, thrombosis) • Brain hemorrhage, usually caused by an aneurysm or poorly controlled hypertension http://www.nhlbi.nih.gov/health/health-topics/topics/atherosclerosis/ http://catalog.nucleusinc.com/generateexhibit.php?ID=10084
Mechanisms of Ischemic Injury • Loss of high-energy compounds • Acidosis due to anaerobic generation of lactate • No reflow due to swelling of astrocytes w/ compression of brain capillaries
Calcium Homeostasis • Normally maintained at 10,000 : 1 in extracellular: intracellular ratio, maintained by at least 4 mechanisms: • Active extrusion of calcium ions from cell by an ATP-driven membrane pump • Exchange of calcium for sodium at the cell membrane due to sodium concentration gradient and the Na+-K+ pump • Sequestration of intracellular Ca2+ in endoplasmic reticulum by an ATP-driven process • Accumulation of intracellular Ca2+ in mitochondria by an oxidant-dependent sequestration
Main Mechanisms • Loss of high energy compound production Cellular calcium imbalance Membrane phospholipid degradation and loss • Ischemia (lack of O2) Decreased aerobic phosphorylation Free radicals
Calcium Imbalance • Calcium derangements lead to a cascade of events: • Activate membrane phospholipases and protein kinases • Production of free fatty acids (FFA’s), including arachidonicacids (AA) • AA lead to the production of leukotrienes and thromboxanes, which are tissue irritants resulting in platelets aggregation, clotting, vasospasm, and edema • Membrane phospholipases also degrade membrane and diminishes the ability of Ca2+ pumps to pump Ca2+ back out of the cell, worsening the cycle.
Free Radicals • Hydrolysis of ATP via AMP lead to an accumulation of hypoxanthine • Increase in intracellular Ca2+ enhances conversion of xanthine dehydrogenase (XD) to xanthine oxidase (XO) • Upon reperfusion or introduction of O2, xanthine oxidase converts hypoxanthine to xanthine and superoxide: • hypoxanthine + O2 xanthine + superoxide • Haber-Weiss Reaction: • O2+ H2O-Fe3 O2 + 2OH-
Lactic Acidosis • Occurs because cells must rely on anaerobic ATP synthesis pathways • These pathways produce lactic acid as end products which are only cleared in the presence of oxygen into a molecule usable in an aerobic pathway, for example lactic acid is cycled back into pyruvate to be eventually used in the Kreb’scycle • Buildup of lactic acid causes the physiological pH to drop resulting in two major issues • Mitochondrial damage and inactivation • Increase in the release of iron containments which leads to the generation of free radicals
Mitochondrial Dysfunction • A result of uncontrolled ion gradients, the mitochondrial membrane becomes distorted/depolarized • Pathways include uncontrolled calcium concentrations within the mitochondria linked with free radicals by impairing the Electron transport chain’s ability to reduce oxygen properly • Results in neuronal damage; being a synthesizer of high energy molecules mitochondria dysfunction means lower amounts of energy to feed neurons and its related regulations leading to damage and eventual cell death in prolonged cerebral ischemia • Can also lead to cell death by because the dysfunctional mitochondria itself releases cytochrome c into the cytosol – inducing cell death
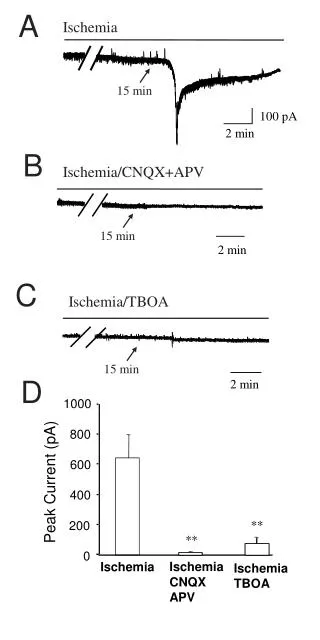
Exitotoxicity • This occurs because calcium that is sequestered in the cell or in the extra cellular matrix can now freely move into intracellular space which results in the release of vesicles containing neurotransmitters such as glutamate • This can lead to nerve cell damage and even possibly cell death by over stimulation • Examples of receptors that are over stimulated by the excessive amount of glutamate are NMDA (N-methyl-D-aspartate) and AMPA (alpha-amino-hydroxy-5-methyl-4-isoxazole proprionic acid) receptors
Interventions 1. Surgery • Post-insult treatment • Carotid endarterectomy: Surgical procedure to unblock carotid artery • Removal of aneurysm hemorrhages close to cranial surface • Cerebral angioplasty widens blood vessels with the use of a small metal coil 2. Thrombolytic Therapy • Emergency acute ischemic stroke treatment • Tissue plasminogen activator (t-PA) used to dissolve clot and returns blood flow
Interventions Cont’d 3. Nutritional Antioxidants • Pre- and Post- Insult treatment • Free radical damage associated with ischemia injury can be reduced or eliminated • Vitamin E, Selenium, Vitamin C, and Beta Carotene leads to Increased Glutathione levels 4. Mitochondrial Dysfunction • Post- Insult treatment • Acetyl-l-carintine transports acetyl-coA outside of mitochondria thus increasing glucose metabolism • Crosses blood brain barrier, preventing brain deterioration and mitochondrial rehabilitation
Interventions Cont’d Cont’d 5.Excitotoxicity Prevention • NMDA Receptor Inhibiting drugs • Requires binding of glutamate or aspartate and co-agonist glycine for efficient opening of ion channel • Competitive Antagonist • Glycine Antagonist • Noncompetitive Antagonist • Uncompetitive Antagonist 6. Therapeutic Hypothermia • Lowers body temperature to prevent tissue damage • 10-12minutes periods post • Suppress acidosis, prevent glutamate release, free radical production and BBB disruption
Cerebral Ischemia - Summary Slide • Insufficient blood flow to brain inability to meet metabolic needs hypoxia • Focal ischemia and global ischemia • Symptoms: blindness, weakness in limbs and body, dizziness, double vision, vertigo, slurred speech, loss of coordination • Causes: atherosclerosis, brain hemorrhage • Ischemic mechanisms: • Loss of high energy compounds Cellular calcium derangements membrane phospholipid degradation and loss • Ischemia (lack of O2) Decrease rate of oxidative phosphorylation Free radicals • Cellular calcium derangements: • Cellular calcium activates membrane phosphatases and protein kinases, which produces free fatty acids such as arachidonic acid, which results in end products such as leukotrienes and thromboxanes as tissue irritants. • Hypoxanthine + O2 xanthine + superoxide, (xanthine oxidase) • Xanthine reductase is converted to xanthine oxidase by increased intracellular calcium, and xanthine oxidase converts hypoxanthine, a product of ATP hydrolysis to xanthine and superoxide • Haber-Weiss Reaction: • O2 + H2O-Fe3 O2 + 2OH- • Mitochondrial structure is changed d to physiological changes resulting in reduced ATP production and cell damage/death • Excessive release of excitatory neurotransmitters over activates neurons leaving to cell damage/death • Interventions includes surgery, thrombolytic therapy, nutritional antioxidants, mitochondrial dysfunction recovery, excitotoxicity prevention and therapeutic hypothermia
References • F, S. (2010, April 14). What Are The Treatments For Cerebral Ischemia? Livestrong.com. Retrieved November 22, 2012, from http://www.livestrong.com/article/204831-what-are-the-treatments-for-cerebral-ischemia/ • Hinds, C. J. (1985, September 21). Prevention and treatment of brain ischemia. British Medical Journal. Retrieved November 22, 2012, from www.ncbi.nlm.nih.gov/pmc/articles/PMC1417168/pdf/bmjcred00466-0004.pdf • Shinji, N., Masaaki, U., Koichi, S., Satoshi, G., Motohiro, M., & Yukitaka, U. (n.d.). Pathophysiology and treatment of cerebral ischemia. The Journal of Medical Investigation. Retrieved November 22, 2012, from http://medical.med.tokushima-u.ac.jp/jmi/vol45/text/v45_n1-4_p057.html • Humes, H.D., Nguyen, V.D., & Hunt, D.A. (1986). High energy phosphates, phospholipids, and calcium in ischemic renal tubular cell injury. Pubmed. • Darwin, M. (1995). The pathophysiology of ischemic injury. • Retrieved from http://www.alcor.org/Library/html/ischemicinjury.html • Klasco, R. (2011, May 02). What is ischemia?. Better Medicine. • Retrieved from http://www.localhealth.com/article/ischemia • Kulick, D. L. (2011). Transient ischemic attack. • Retrieved from http://www.medicinenet.com/transient_ischemic_attack_tia_mini-stroke/page2.htm