Download
1 / 68
690 likes | 848 Views
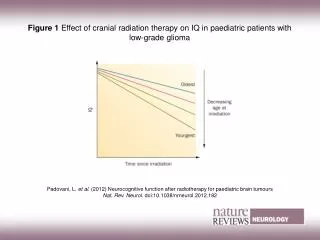
management of low grade glioma. robert r johnson , m.d. department of radiation oncology august 4, 2011. table of contents. background pathological classification m olecular features presentation treatment sequelae future directions. background. slow-growing tumors

E N D
management of low grade glioma robert r johnson, m.d. department of radiation oncology august 4, 2011
table of contents background pathological classification molecular features presentation treatment sequelae future directions
background • slow-growing tumors • 10% of primary brain tumors in adults • 20-25% of gliomas • 2000 cases/year in u.s. • divided into: • pilocyticastrocytoma • diffusely infiltrating glioma
background • pilocyticastrocytoma • more common in children (jpa) • cerebellum • do occur in young adults • low grade • even after recurrence • cured by surgery • > 90% long-term survival after complete resection • 70-80% after incomplete resection
background • diffusely infiltrating glioma • 3rd-4th decade of life • 20 years earlier than high-grade gliomas • slow growing but eventually fatal • 80% transform to high-grade
histological subtypes astrocytoma – 50% oligodendroglioma – 28% oligoastrocytoma – 22%
prognosis • central brain tumor registry of u.s. (cbtrus) • 42,688 patients diagnosed between 1995-2006 • astrocytoma • 5-year survival 47% • oligoastrocytoma • 5-year survival 57% • oligodendroglioma • 5-year survival 79% http://cbtrus.org/2010-NPCR-SEER/Table23.pdf
pathological classification • who grading • I: slow-growing, non-malignant • pilocyticastrocytoma • II: relatively slow-growing, can recur as higher-grade tumor • astrocytoma, oligodendroglioma, oligoastrocytoma
pathological classification • stanne-mayo classification • based on 4 criteria: • nuclear atypia • mitoses • endothelial proliferation • necrosis • grade I: 0/4 • pilocyticastrocytoma • grade II: 1/4 • astrocytoma, oligodendroglioma, oligoastrocytoma
molecular features • ploidy • better prognosis with diploid relative to aneuploid • proliferation • better prognosis with ki-67 index < 3% • co-deletion of 1p and 19q • better prognosis
co-deletion of 1p/19q • found in 70-75% oligodendroglioma • 35-40% oligoastrocytoma • rarely in pure astrocytoma • favorable prognosis • 139 samples of 80 patients with low-grade glioma • median survival: • 15 years with co-deletion • 5 years without • more likely to respond to chemotherapy
imaging • pilocyticastrocytoma • well-circumscribed • cystic • contrast-enhancing • vasogenic edema is rare
imaging • diffusely infiltrating glioma • ct • diffuse , non-enhancing • calcifications with oligodendroglioma
imaging • diffusely infiltrating glioma • mri • hypointense and non-enhancing on t1 • hyperintense on t2
treatment • pilocyticastrocytoma • more amenable to total resection • well-circumscribed • close follow-up after surgery • 70-80% long-term survival after subtotal resection • transformation to high-grade glioma very rare • adjuvant radiotherapy not typically offered • 50-55 gy for recurrent/unresectable disease
pilocyticastrocytoma • 20 adults from ncctg 86-72-51 followed prospectively • 3 patients irradiated after biopsy • 50.4 gy • 17 patients observed after subtotal or gross total resection brown et al. ijrobp 2004;58:1153-1160.
pilocyticastrocytoma • excellent prognosis irrespective of treatment modality • distinctly different behavior from diffusely infiltrating gliomas • 10-year survival 95% vs 17% in ncctg 86-72-51
diffusely infiltrating glioma surgery radiation chemotherapy
surgery • usually performed first • establish diagnosis • tumor debulking • total resection uncommon due to diffuse infiltration • rarely curative • retrospective data suggests benefit for total/subtotal resection • most accurate pathological assessment
radiation • 3 randomized trials have assessed timing and dose of adjuvant radiotherapy • eortc 22485 • immediate vs delayed • eortc 22484 • 45 gyvs 59.4 gy • ncctg 86-72-51 • 50.4 gyvs 64.8 gy
eortc 22485 • 314 patients with resected or biopsied low-grade glioma • inclusion criteria • supratentorial low-grade glioma • 16-65 years • randomized to 54 gy/30 fractions vs observation and radiation at progression van den bent et al. lancet 2005;366:985-990.
eortc 22485 • 65% patients in observation group treated with radiation at recurrence • median survival after recurrence 3.4 years vs 1.0 years • favoring observation group • ~70% histologically confirmed recurrences high-grade • no quality of life study
eortc 22485 • conclusions • no difference in overall survival for early vs delayed radiotherapy • longer time to recurrence with early rt • unknown if rt or recurrence is worse for quality of life • seizures at 1 year • 25% with rt, 41% with observation • P = 0.03
eortc 22484 • 379 patients with resected or biopsied low-grade glioma • inclusion criteria • supratentorial low-grade glioma • incompletely resectedpilocyticastrocytoma • 16-65 years • randomized to 45 gy/25 fractions vs 59.4 gy/33 fractions karim et al. ijrobp 1996; 36:549-556.
eortc 22484 5 year os 58% vs 59% 5 year pfs 47% vs 50%
eortc 22484 • interesting subgroup analyses • extent of resection • size of tumor
eortc 22484 no dose response seen
eortc 22484 • acute toxicity more common in high-dose arm • 15% vs 8% required > 1 week break • no difference in late toxicity • no radionecrosis in either arm
eortc 22484 • conclusions • no dose response above 45 gy • prognostic importance of • age • extent of resection • tumor size • histology • astrocytoma worst • neurological deficits
eortc 22484/22485 • poor prognostic variables • age > 40 • tumor > 6 cm • tumor crossing midline • astrocytoma histology • neurological deficits • 0-2 = low risk, median survival 7.7 years • > 3 = high risk, median survival 3.2 years
ncctg 86-72-51 • 203 patients with resected or biopsied low-grade glioma • inclusion criteria • supratentorial low-grade glioma • pilocyticastrocytoma excluded • > 18 years • randomized to 50.4 gy/28 fractions vs 64.8 gy/36 fractions shaw et al. jco 2002;20:2267-2276.
ncctg 86-72-51 • toxicity • grade 3-5 toxicity seen in 13% patients on both arms • radionecrosis and encephalitis • 5% vs 2.5% at 2 years • more common with high dose
ncctg 86-72-51 • conclusions • no dose response above 50.4 gy • higher severe toxicity with high dose • prognostic importance of • extent of resection • tumor size • histology • astrocytoma worst • age
radiation • conclusions • no difference in survival with post-op rtvsrt at progression • improved pfs • no dose response above 45-50 gy • increased toxicity with higher dose • age, histology, tumor size, extent of resection all predict outcome
chemotherapy no clearly established role pcv (procarbazine, ccnu, vincristine) and temozolomide been evaluated in several studies
rtog 98-02 • 251 patients • 3 armed trial • arm 1: low risk (age < 40, gross total resection) • observe • arms 2 and 3: high risk (age > 40, subtotal resection or biopsy) • randomized to 54 gy +/- 6 cycles adjuvant pcv • procarbazine, ccnu, vincristine • preliminary results presented at asco in 2006
rtog 98-02 • final results presented at asco in 2008 • rt + chemo arm better for all endpoints • median os • not reached vs 7.5 years (ns) • median pfs • not reached vs 4.4 years (p = 0.005) • analyses of 1p/19q status forthcoming
temozolomide • significant survival benefit when used concurrently with radiotherapy in glioblastomamultiforme • stupp trial • easy administration • good toxicity profile
temozolomide • danafarber/brigham and women’s cancer center • 44 patients with • newly diagnosed oligoastrocytoma or oligodendroglioma • recurrent low-grade glioma • 6 cycles or tumor progression or toxicity kesari et al. clinical cancer research 2009;15:330-337
temozolomide • 95% disease control rate • 20% partial response • 75% stable disease • >72 month median survival • 38 month median progression-free survival
temozolomide • significantly better survival for • mgmt promoter methylation • > 72 months with, 29 months without • 1p/19q co-deletion • > 72 months with, 27 months without • toxicity mild