Download
1 / 56
560 likes | 654 Views
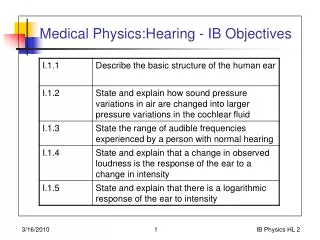
Medical Literature-Based Objectives 1. List the Landmark Radiographic Studies for acute PE evaluation 2. Understand the role of Clinical Decision Rules in acute PE evaluation 3. Consider Special Cases of acute PE - COPD - Pregnancy - IVC Filters - Submassive PE.

E N D
Medical Literature-Based Objectives 1. List the Landmark Radiographic Studies for acute PE evaluation 2. Understand the role of Clinical Decision Rules in acute PE evaluation 3. Consider Special Cases of acute PE - COPD - Pregnancy - IVC Filters - Submassive PE
Ventilation Perfusion Mismatch
Value of the Ventilation/Perfusion Scanin Acute Pulmonary EmbolismResults of the Prospective Investigation ofPulmonary Embolism Diagnosis (PIOPED)The PIOPED Investigators JAMA. 1990;263:2753-2759
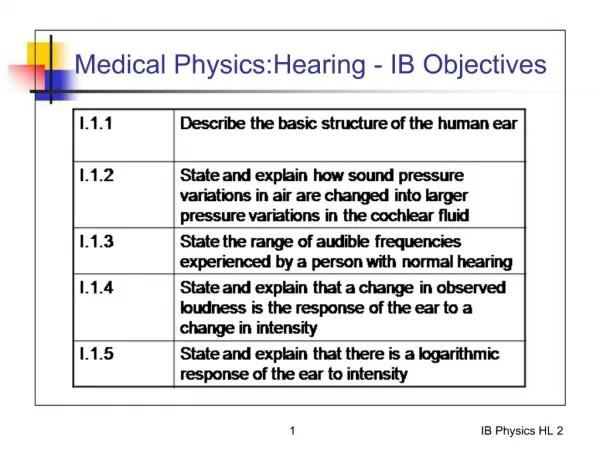
Table 1. —PIOPED Central Scan Interpretation Categories and Criteria High probability >=2 Large (>75% of a segment) segmental perfusion defects without corresponding ventilation or roentgeno- graphic abnormalities or substantially larger than either matching ventilation or chest roentgenogram abnormalities >=2 Moderate segmental (>25% and <= 75% of a segment) perfusion defects without matching ventilation or chest roentgenogram abnormalities and 1 large mismatched segmental defect >= 4 Moderate segmental perfusion defects without ventilation or chest roentgenogram abnormalities Intermediate probability (indeterminate) Not falling into normal, very-low-, low-, or high-probability categories Borderline high or borderline low Difficult to categorize as low or high Low probability Nonsegmental perfusion defects (e.g., very small effusion causing blunting of the costophrenic angle, cardiomegaly, enlarged aorta, hila, and mediastinum, and elevated diaphragm) Single moderate mismatched segmental perfusion defect with normal chest roentgenogram Any perfusion defect with a substantially /larger chest roentgenogram abnormality Large or moderate segmental perfusion defects involving no more than 4 segments in 1 lung and no more than 3 segments in 1 lung region with matching ventilation defects either equal to or larger in size and chest roentgenogram either normal or with abnormalities substantially smaller than perfusion defects >3 Small segmental perfusion defects (<25% of a segment) with a normal chest roentgenogram Very low probability <=3 Small segmental perfusion defects with a normal chest roentgenogram Normal No perfusion defects present Perfusion outlines exactly the shape of the lungs as seen on the chest roentgenogram (hilar and aortic impressions may be seen, chest roentgenogram and/or ventilation study may be abnormal)
ESTABLISHED IN 1812 JUNE 1, 2006 VOL. 354 NO. 22 Multidetector Computed Tomography for Acute Pulmonary Embolism Paul D. Stein, M.D., Sarah E. Fowler, Ph.D., Lawrence R. Goodman, M.D., Alexander Gottschalk, M.D., Charles A. Hales, M.D., Russell D. Hull, M.B., B.S., M.Sc., Kenneth V. Leeper, Jr., M.D., John Popovich, Jr., M.D., Deborah A. Quinn, M.D., Thomas A. Sos, M.D., H. Dirk Sostman, M.D., Victor F. Tapson, M.D., Thomas W. Wakefield, M.D., John G. Weg, M.D., and Pamela K. Woodard, M.D., for the PIOPED II Investigators The NEW ENGLAND JOURNAL of MEDICINE
64-year-old woman with pulmonary embolism Kluge A et al. AJR 2006;186:1686-1696
Annals of Internal Medicine Gadolinium-Enhanced Magnetic Resonance Angiography forPulmonary EmbolismA Multicenter Prospective Study (PIOPED III)Paul D. Stein, MD; Thomas L. Chenevert, PhD; Sarah E. Fowler, PhD; Lawrence R. Goodman, MD; Alexander Gottschalk, MD;Charles A. Hales, MD; Russell D. Hull, MBBS, MSc; Kathleen A. Jablonski, PhD; Kenneth V. Leeper Jr., MD; David P. Naidich, MD;Daniel J. Sak, DO; H. Dirk Sostman, MD; Victor F. Tapson, MD; John G. Weg, MD; and Pamela K. Woodard, MD, for the PIOPED III(Prospective Investigation of Pulmonary Embolism Diagnosis III) Investigators*ann intern med 2010: 152:434
Table 1. Reference Test Basis for Diagnosis or Exclusion of PE in Patients Who Had Magnetic Resonance Angiography Criteria Patients, n (%) Diagnosis of PE CT angiogram showing PE in a main or lobar pulmonary artery 94 (90) CT angiogram showing PE in a segmental or subsegmental 8 (8) pulmonary artery in a patient with high clinical 2 (2) probability according to the Wells criteria High-probability VQ lung scan in a patient with no previous PE and high or intermediate probability according to the Wells criteria Total 104 (100) Exclusion of PE Normal D-dimer (D-dimer level 500 ng/mL) in a patient with low or intermediate probability according to the Wells criteria 95 (36) Negative CT angiogram in a patient with low probability 132 (49) according to the Wells criteria Negative CT angiogram and CT venogram or venous 34 (13) ultrasonogram in a patient with intermediate probability according to the Wells criteria Normal VQ lung scan 6 (2) Total 267 (100)
Table 3. Results of MRA and Combined MRA and MRV, by Reference Test Test Result Reference Test Result, n Total, n Positive Negative for PE for PE MRA result Positive 59 2 61 Negative 17 201 218 Technically inadequate 28 64 92 Total 104 267 371 MRA and MRV result Positive 65 4 69 Negative 6 101 107 Technically inadequate 33 161 194 Total 104 266 370 MRA magnetic resonance angiography; MRV magnetic resonance venography; PE pulmonary embolism.
Table 5. Recruited Patients and Technical Adequacy, Sensitivity, and Specificity of Combined Magnetic Resonance Angiography and Venography by Clinical Center Clinical Recruited Technically Inadequate Sensitivity [95% CI], n/N (%) Specificity [95% CI], n/N (%) Center Patients, n [95% CI], n/N (%) 1 68 43/68 (63 [52–75]) 5/6 (83 [36–100]) 17/19 (89 [67–99]) 2 41 26/41 (63 [49–78]) 6/6 (100 [54–100]) 9/9 (100 [66–100]) 3 59 21/59 (36 [23–49]) 21/22 (95 [77–100]) 15/16 (94 [70–100]) 4 77 43/77 (56 [45–67]) 1/1 (100 [3–100]) 32/33 (97 [84–100]) 5 53 25/53 (47 [34–60]) 14/17 (82 [57–96]) 11/11 (100 [72–100]) 6 37 10/37 (27 [13–41]) 13/13 (100 [75–100]) 14/14 (100 [77–100]) 7 35 26/35 (74 [60–89]) 5/6 (83 [36–100]) 3/3 (100 [29–100]) Total 370 194/370 (52 [47–58]) 65/71 (92 [83–97]) 101/105 (96 [91–99])
Context Is gadolinium-enhanced magnetic resonance pulmonary angiography a feasible and accurate test for diagnosing acute PE? Contribution Magnetic resonance angiography was technically inadequate in 25% of the 371 patients who had the test and identified 57% of the 104 patients with embolism. The sensitivity and specificity of technically adequate tests were 78% and 99%. Caution In this multicenter study, many patients with suspected pulmonary embolism were ineligible or declined participation. Implication Because magnetic resonance pulmonary angiography is often technically inadequate, consider the test only at centers that routinely perform it well and only for patients with contraindications to standard tests. —The Editors
Performance of 4 Clinical Decision Rules in the Diagnostic Management of Acute Pulmonary Embolism A Prospective Cohort Study from the Promethius Study Group Ann Intern Med. 2011;154(11):709-718.
Performance of 4 Clinical Decision Rules in the Diagnostic Management of Acute Pulmonary Embolism A Prospective Cohort Study from the Promethius Study Group Ann Intern Med. 2011;154(11):709-718 CDR = clinical decision rule
Performance of 4 Clinical Decision Rules in the Diagnostic Management of Acute Pulmonary Embolism A Prospective Cohort Study from the Promethius Study Group Ann Intern Med. 2011;154(11):709-718
Performance of 4 Clinical Decision Rules in the Diagnostic Management of Acute Pulmonary Embolism A Prospective Cohort Study from the Promethius Study Group Ann Intern Med. 2011;154(11):709-718. Accuracy Indexes of the Clinical Decision Rules in Combination With a Normal d-Dimer Result in Patients With a Suspected Event
Context • Several clinical decision rules (CDRs) are available to evaluate patients with possible pulmonary embolism (PE). It is not known which CDR, if any, is best to use. • Contribution • In this multicenter, prospective study, 4 CDRs were used to determine whether PE was likely or unlikely, combined with the results of d-dimer testing, and did equally well at excluding PE or indicating the need for further testing. The CDRs were the Wells rule, the revised Geneva score, the simplified Wells rule, and the simplified revised Geneva score. • Implication • Provided that these 4 CDRs are used correctly, clinicians can confidently choose them according to personal or institutional preferences to assist in the evaluation of possible PE. • —The Editors
Pulmonary Embolism in Patients with Unexplained Exacerbation of Chronic Obstructive Pulmonary Disease: Prevalence and Risk Factors Isabelle Tillie-Leblond, MD, PhD; Charles-Hugo Marquette, MD, PhD; Thierry Perez, MD; Arnaud Scherpereel, MD, PhD; Christophe Zanetti, MD; André-Bernard Tonnel, MD, PhD; and Martine Remy-Jardin, MD, PhD Ann Intern Med. 21 March 2006;144(6):390-396
Context Pulmonary embolism (PE) is common in patients with COPD exacerbations; The 2 conditions present similarly. Content For 45 months, every patient presenting with severe COPD exacerbation of unknown cause received an evaluation for PE that included a spiral computed tomography scan and color Doppler ultrasonography of the legs. Cautions This was a single-center study.
Pulmonary Embolism in Patients with Unexplained Exacerbation of Chronic Obstructive Pulmonary Disease: Prevalence and Risk Factors Ann Intern Med. 2006;144(6):390-396. Results of Spiral Computed Tomography Angiography in Patients Initially Referred for Suspected Acute Pulmonary Embolism
Context Pulmonary embolism (PE) is common in patients with COPD exacerbations; the 2 conditions present similarly. Content For 45 months, every patient presenting with severe COPD exacerbation of unknown cause received an evaluation for PE that included a spiral computed tomography scan and color Doppler ultrasonography of the legs. -Twenty-five percent of 197 patients had PE. -Malignant disease, history of VTE, and a decrease in PaCO2 level from baseline were the only factors associated with PE. Cautions This was a single-center study. Implications We need additional studies to confirm the high prevalence of PE in unexplained severe exacerbations of COPD and to study the value of routine testing for PE in patients with this clinical presentation. —The Editors
Estimated radiation absorbed by fetus in procedures for diagnosing PE The Task Force for the Diagnosis and Management of Acute Pulmonary Embolism for the European Society of Cardiology European Heart Journal 2008 __________________________________________________________ Test Estimated radiation uGymSv ……………………………………………………………………………………………... Chest radiography <10 0.01 Perfusion lung scan with technetium 60–120 0.06–012 99m-labelled albumin V/Q scan 200 0.2 CT angiography First trimester 3–20 0.003–0.02 Second trimester 8–77 0.008–0.08 Third trimester 51–130 0.051–0.13 Pulmonary angiography by femoral 2210–3740 2.2–3.7 access Pulmonary angiography by brachial <500 <0.5 access Exposure to less than 5 rem (50 mSv) has not been associated with an increase in fetal anomalies orpregnancy loss (American College of Obstetricians 2004).
Advantages and disadvantages of imaging techniques in pregnancy Ventilation perfusion scan Advantages • Low radiation exposure to breast • Low radiation exposure to fetus • High rate of normal scans in pregnancy, 70% Disadvantages • Interpretation of test strongly linked to clinical pretest probability. No clinical decision rules validated in pregnancy • Does not offer alternative diagnosis • No accuracy studies in pregnancy available thelancet.com Vol 375 February 6, 2010
Advantages and disadvantages of imaging techniques in pregnancy CT pulmonary angiography Advantages • Could offer an alternative diagnosis • Low radiation exposure to fetus • Better availability than ventilation perfusion scan • More cost effective than other approaches Disadvantages • Radiation exposure to breast (can be reduced with breast shields) • Technical limitations in pregnancy. Need to modify imaging and injection protocol • No accuracy or outcome studies available • High rate of detection of subsegmental emboli (the clinical significance of subsegmental emboli is unclear, so the rate of detection needs to be low) • Theoretical concern about the effect of iodinated contrast on fetal thyroid thelancet.com Vol 375 February 6, 2010
Advantages and disadvantages of imaging techniques in pregnancy MRI Advantages • No ionising radiation involved • Misses subsegmental emboli Disadvantages • Insufficient accuracy or outcome data • Most widely used protocols involve gadolinium (which crosses the placenta), for which insufficient fetal safety data are available thelancet.com Vol 375 February 6, 2010
Advantages and disadvantages of imaging techniques in pregnancy Compression ultrasonography Advantages • No exposure to radiation • Non-invasive Disadvantages • Possible low sensitivity in patients without signs and symptoms of deep vein thrombosis thelancet.com Vol 375 February 6, 2010
Kaplan-Meier analysis of time to PE over an 8 year period after index thromboembolic event The PREPIC Study Group, Circulation 2005 The PREPIC Study Group, Circulation 2005 The PREPIC Study Group, Circulation 2005 The PREPIC Study Group, Circulation 2005
Massive Pulmonary Embolism - ICOPERKucher N, Goldhaber S., et al. Circulation 2006 Overall mortality (A) and cardiovascular mortality (B) in 11 patients with massive PE who received an IVC filter and in 97 patients with massive PE who did not receive an IVC filter
MASSIVE ACUTE PE Most clinicians would not withhold fibrinolyticsfrom patients with acute PE and hypotension due to overt RV failure
Should Right Ventricular Dysfunction Post- Acute PE be Treated Any Differently? SUBMASSIVE ACUTE PE Pulmonary hypertension or right ventricular dysfunction without hypotension or shock
Risk factors and coexisting disorders __________________________________________________________________________________________________________________ Variable Yes No Missing Overall __________________________________________________________________________________________________________________ Diagnosis of deep-vein thrombosis 1205 1237 12 49·3% Body-mass index ≥29 kg/m2 571 1384 499 29·2% Surgery within 2 months 708 1742 4 28·9% Bed rest ≥5 days 675 1723 56 28·1% Previous deep-vein thrombosis or PE 592 1784 78 24·9% Cancer 551 1894 9 22·5% Current cigarette smoking 403 1878 173 17·7% Chronic obstructive pulmonary disease 303 2138 13 12·4% Trauma 274 2179 1 11·2% Clinical congestive heart failure 256 2179 19 10·5% Current central-venous catheter 183 2266 5 7·5% Left-ventricular ejection fraction <0·4 118 1778 558 6·2% Current chemotherapy 130 2317 7 5·3% Known hypercoagulable state 117 2121 216 5·2% Creatinine >177 μmol/L 125 2313 16 5·1% Platelets <100×109/L 108 2331 15 4·4% Active bleeding requiring transfusion 60 2386 8 2·4% Previous intravenous coagulation filter 21 2427 6 0·9% Acute pulmonary embolism: clinical outcomes in the International Cooperative Pulmonary Embolism Registry (ICOPER)Samuel Z Goldhaber, Luigi Visani, Marisa De RosaLancet 1999; 353: 1386–89
Acute pulmonary embolism: clinical outcomes in the International Cooperative Pulmonary Embolism Registry (ICOPER)Samuel Z Goldhaber, Luigi Visani, Marisa De Rosa, for ICOPER. Lancet 1999; 353: 1386–89 Cumulative mortality according to status of right-ventricular function on baseline echocardiogram
Variable Hazard ratio (95% CI) _____________________________________ _______________________ Age >70 years 1·6 (1·1–2·3) Cancer 2·3 (1·5–3·5) Clinical congestive heart failure 2·4 (1·5–3·7) COPD 1·8 (1·2–2·7) Systolic blood pressure <90 mm Hg 2·9 (1·7–5·0) Respiratory rate <20/min 2·0 (1·2–3·2) Right-ventricular hypokinesis 2·0 (1·3–2·9) Final model (815 patients) Acute pulmonary embolism: clinical outcomes in the International Cooperative Pulmonary Embolism Registry (ICOPER)Samuel Z Goldhaber, Luigi Visani, Marisa De Rosa, for ICOPER. Lancet 1999; 353: 1386–89
Survival through 30 days in 1035 patients with PE and systolic arterial BP >= 90 mm Hg at presentation, according to the presence or absence of right RV hypokinesis on the baseline echocardiogram (adjusted for cancer, congestive heart failure, chronic lung disease, and age) Kucher, N, Goldhaber S, et al. Arch Intern Med 2005 Kucher, N, Goldhaber S, et al. Arch Intern Med 2005
Cumulative incidence of recurrent venous thromboembolism Grifoni, S. et al. Arch Intern Med 2006
Follow-up Outcomes in Study Patients Based on In-Hospital Course of Right Ventricular Dysfunction (RVD) No RVD RVD Regression RVD Persistence Outcome (n=155) (n=87) (n=59) Recurrent VTE PE-related death Fatal and nonfatal PE Death 3 (3) 0 2 (2) 11 (13) 15 (10) 2 (1) 6 (4) 21 (15) 14 (24) * 6 (10) * 12 (20) * 13 (24) * P<.05 vs the other 2 groups by Fisher exact test. Grifoni S, et al. Arch Intern Med 2006
Guidelines on the diagnosis and management of acute pulmonary embolism. The Task Force for the Diagnosis and Management of Acute Pulmonary Embolism for the European Society of Cardiology. European Heart Journal 2008 Major trials reporting definitions and prognostic significance of RV dysfunction assessed by echocardiography in acute pulmonary embolism ___________________________________________________________________________________________________ Author n Patient characteristics Echocardiographic criteria Early mortality RVD(1) vs. RVD( – ) …………………………………………………………………………………………………………………………………………………………………………………………….. Goldhaber et al. 101 Normotensive RV hypokinesis 4.3 vs. 0% and dilatation Ribeiro et al. 126 Normotensive and hypotensive RVD 12.8 vs. 0% Kasper et al. 317 Normotensive and hypotensive RV >30 mm or TI >2.8 m/s 13 vs. 0.9% Grifoni et al. 162 BP >=100 mmHg At least one of the following: 4.6 vs. 0% RV >30 mm or RV/LV>1 Paradox septal systolic motion AcT<90 ms or TIPG >30 mmHg Kucher et al. 1035 BP >=90 mmHg RVD 16.3 vs. 9.4% All data refer to in-hospital PE-related mortality, except a 30 day all-cause mortality. RVD(+) = patients with RV dysfunction; RVD( – ) = patients with normal RV function. TI = tricuspid insufficiency; AcT = acceleration time of right ventricular ejection; TIPG = tricuspid insufficiency peak gradient.
In-Hospital Clinical Events, no. (%) for Patients with Acute Submassive PE Heparin Plus Heparin Plus Alteplase Placebo Event (N=118) (N=138) ‘P’ Value Death, all causes 4 (3.4) 3 (2.2) 0.71 Escalation of treatment 12(10.2) 34(24.6) 0.004 (catecholamines, repeat thrombolysis, intubation, CPR, embolectomy) Secondary endpoints Recurrent PE 4(3.4) 4 (2.9) 0.89 Major bleeding 1 (0.8) 5 (3.6) 0.29 Ischemic stroke 0 1 (0.7) 1.0 Konstantinides, S et al. N Engl J Med 2002