Download

1 / 65
650 likes | 797 Views
The implementation of classification of acute low back pain patients in physical therapy: An analysis of practice. Britt Smith MSPT, OCS, FAAOMPT Julie Whitman DSc, DPT, OCS, FAAOMPT Marcia Smith PhD, PT. The societal burden of LBP in Western Culture is significant. {Waddell, 1996}.

E N D
The implementation of classification of acute low back pain patients in physical therapy: An analysis of practice Britt Smith MSPT, OCS, FAAOMPT Julie Whitman DSc, DPT, OCS, FAAOMPT Marcia Smith PhD, PT
The societal burden of LBP in Western Culture is significant. {Waddell, 1996} • Back pain accounts for 7% of the visits to general practices {Croft, 1998; Croft, 2006}, making it the 5th most common reason a person visits their doctor in the US. • Frymoyer & Durrett estimated the direct medical cost of LBP in the United States was $33 billion in 1994, and direct with indirect costs estimates range from $50 billion to $100 million. {Frymoyer & Durrett, 1991} • Maetzel & Li reviewed the economic impact of LBP on society and estimated that the indirect costs are upwards of 3x higher than direct cost.{Maetzel & Li, 2002} • Katz confirms these estimates with an updated estimate of total cost of low back pain (LBP) at $100-200 billion dollars a year in the United States. {Katz, 2006}
Carey et al demonstrated that cost is not linked to outcomes. • Carey et alfound similar outcomes between general practitioners, chiropractors and orthopaedic surgeons with wide variance of cost, with GPs in an HMO being the cheapest and surgeons most expensive.{Carey et al, 1995} • The United States has the highest rates world-wide for disc surgeries, with marginal cost-effectiveness as expressed for QALYs (Quality Adjusted Life Year): ranging from $34,000/QALY for a discectomy to $3,000,000/QALY for instrumentation in fusion for degenerative spondylolisthesis with stenosis. {Katz, 2006}
Non-surgical options are less costly; however, the evidence for effectiveness of most of these procedures is weak or no evidence is available.
Cochrane reviews • Back school (education) • Exercise and non-specific LBP • Massage • Manipulation • Traction
Back school (education): • “There is conflicting evidence whether back schools are more effective than placebo or waiting list controls for pain, function and return-to-work. There is moderate evidence suggesting that back schools, in an occupational setting, reduce pain, and improve function and return-to-work status, in the short and intermediate-term, compared to exercises, manipulation, myofascial therapy or advice, placebo or waiting list controls, for patients with chronic LBP.”{Heymans et al, 2005}
Exercise and non-specific LBP: • “Exercise therapy appears to be slightly effective at decreasing pain and improving function in adults with chronic low-back pain, particularly in healthcare populations. In subacute low-back pain there is some evidence that a graded activity program improves absenteeism outcomes, though evidence for other types of exercise is unclear. In acute low-back pain, exercise therapy is as effective as either no treatment or other conservative treatments.”{Hayden et al, 2005}
Massage: • ““Massage might be beneficial for patients with subacute and chronic non-specific low-back pain, especially when combined with exercises and education. The evidence suggests that acupuncture massage is more effective than classic massage, but this need confirmation. More studies are needed to confirm these conclusions and to assess the impact of massage on return-to-work, and to measure longer term effects to determine cost-effectiveness of massage as an intervention for low-back pain.”{Furlan et al, 2002}
Manipulation: • “There was little or no difference in pain reduction or the ability to perform everyday activities between people with low-back pain who received spinal manipulation and those who received other advocated therapies. This review of 39 trials found that spinal manipulation was more effective in reducing pain and improving the ability to perform everyday activities than sham (fake) therapy and therapies already known to be unhelpful. However, it was no more or less effective than medication for pain, physical therapy, exercises, back school or the care given by a general practitioner.” {Assendelft et al, 2004}
Traction: • “The evidence suggests that traction is probably not effective. Neither continuous nor intermittent traction by itself was more effective in improving pain, disability or work absence than placebo, sham or other treatments for patients with a mixed duration of LBP, with or without sciatica. Although trials studying patients with sciatica had methodological limitations and inconsistent results, there was moderate evidence that auto-traction was more effective than mechanical traction for global improvement in this population.” {Clarke et al, 2005}
The problem Heterogeneity of subjects in RCTs of LBP Treatment • A central problem with RCTs investigating treatment of low back pain is the heterogeneity of the study population. {Bouter et al, 1998; Leboeuf-Yde et al, 1997}
Subgroup studies greatly enhances RCTs ( & patient care) by identifying homogenous groups • “These types of studies [i.e. matched vs. unmatched treatments in subgroups of patients with non-specific low back pain] may further improve the management of patients with low back pain and better tailor treatment options to the needs of individual patients.” {Koes et al, 2006}
…and Failures of the Pathoanatomical Model • Lutz et al reviewed the diagnoses of LBP reported in a major German medical journal through out the 20th Century. The review clearly demonstrates the collapse of definitive diagnoses ascribed to etiology of LBP in the late century. {Lutz et al, 2004} Etiology of disc pathology
Delitto et al Classification of Acute LBP patients Delitto et al have developed a classification system that is proving to be robust in the development of both RCTs of a more homogenous nature and changing the general practice pattern for physical of LBP. {Delitto et al, 1995}
The classification system developed by Delitto et al.{Delitto et al, 1995} has demonstrated clinical utility: Reliability, efficiency and cost-effectiveness. Reliability • The classification system has demonstrated good reliability {Fritz et al 2006, Brennan et al, 2006; Fritz & George, 2000; Heiss et al, 2004} Effectiveness • Fritz et al examined the effectiveness of treating patients using this classification system compared to AHCPR guidelines treatment directed by physicians.{Fritz et al, 2003} • Matched patients averaged 20% greater reductions in disability (short-term and long-term as measured by the Oswestry) compared to the unmatched groups. {Fritz et al, 2003} • Brennan et al in an RCT randomizing patients to one of 3 subgroups found a 6.6 point difference in the matched groups vs. the unmatched groups. {Brennan et al, 2006} Cost-effectiveness • A recent study examined the outcomes and cost-effectiveness of the treatment of 215 low back pain patients with spinal manipulation.{Fritz et al, 2006} • This retrospective study found the less duration of the episode of care, lower pain and disability scores and reduced cost ($728 vs. $524) in the group treated with spinal manipulation in the subgroup identified by the CPR. {Fritz et al, 2006}
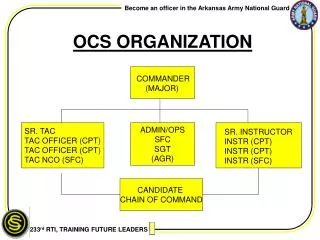
Treatment-Based Classification • Three levels of classification need to be made by the therapist: 1.First Level: Is the patient appropriate for physical therapy management? 2. Second Level: What is the level of acuity? (staging the patient) 3. Third Level: What treatment should be used? (classification)
Medical History Form Modified Oswestry Questionnaire (OSW) Fear-avoidance Beliefs Questionnaire (FABQ) Pain Diagram Screening/Outcome Measures Sorting out red flags & yellow flags
ACUTE LOW BACK PAIN Stage 1: Triage RED FLAGS PHYSICAL THERAPY YELLOW FLAGS
ACUTE LOW BACK PAIN Manipulation Stabilization Spectific Exercise Traction Classification of Acute Low Back Pain Patients
LOW BACK PAIN Manipulation Stabilization Specific Exercises Traction • Primarily unilateral sx • no signs of NR • comp. • (+) SI or lumbar dysfunction Manipulate • Flynn et al. Spine 2002 • Childs et al. Annals Int Med. 2004 • Patient profile • FABQ-w <19 • Pain onset < 16 days • Hypomobile at 1 or more LS seg. • Hip IR >35 degrees (1 or both) • No pain below knee
LOW BACK PAIN Manipulation Stabilization Exercises Specific Exercises Traction Frequent prior episodes frequent SMT, “instability catch” evidence of segmental hypermobility Stabilization Exercises • Hicks et al. Arch Phys Med Rehab. 2005 • Patient profile • Positive PIT test • Aberrant motions • Hypermobility • Younger patient (< 40 years old) • SLR > 91 degrees
LOW BACK PAIN Manipulation Stabilization Exercises Specific Exercises Traction Patient preference for spec postures centralization during exam Preferred Directional Movement • Long et al. Spine. 2005 • Patient profile • Directional movement • Centralization phenonmenon
LOW BACK PAIN Manipulation Stabilization ex Specific Exercises Traction Signs of NR compress. No centralize with mvmt Traction/ Autotraction • No strong evidence of effectiveness (level 5) • Cochrane review of traction: Negative. • Patient profile in this group • Presence of leg pain • Signs of nerve root compression • Either peripheralization with extension OR crossed SLR (Fritz et al 2007)
EOTA (extension oriented treatment group) • Traction Fritz et al 2007
Hypothesis • Utilization of the treatment-based classification of acute low back pain patients into appropriated subgroups will improve the effectiveness and efficiency in the outcomes of LBP patients (i.e. better outcomes with less treatments or less cost allocation). • An physical therapist who has implemented the classification components, as they emerged with research, should demonstrate improved effectiveness, over time, in the treatment of this group of patients (i.e. patients with acute LBP).
Methods • The proposal will require implementing a tracking with the MDS and Excel spreadsheet of patient treatment and outcomes. The prospective data collection is over a 8 week period ending on July 24, 2006. • A retrospective review of 1 therapist’s (BS) patients in 2001 (total of 28 patients), entry of the data on the spread sheet for analysis. This data is a baseline of utilization of the classification (most of the literature is post-2001). • This single subject (BS) will allow for more consistency and validity (i.e. to compare and contrast the various therapists and look for patterns of treatment outcomes with different patient distribution in the clinic (e.g. one therapist mostly works with the Pilates equipment and all of her LBP patients are chronic (100%)) would be difficult. • The project will be expanded to include analysis of the all physical therapists in the practice and examining the effects of introducing the treatment based classification to the other therapists.This data provides a perspective on possible change in outcomes as knowledge of the classification system has matured.
Chronicity of symptoms • Acute/subacute LBP: < 90 days of symptoms • Chronic LBP:> 90 days of symptoms (a convention that 3 months is the treshold for chronicity (very debatable)
Retrospective • 35 charts were randomly selected (alphebetical order, pick every 3rd name). • Data from 28 patients were included in the study. • The charts were reviewed & data recorded for demographics, Rx and outcomes measures.
Prospective • Patients with LBP treated during the period of data collection (consecutive selection) were included. • Data was collected from a total of 26 patients with LBP, who were treated by 1 PT during the period of May 23-July 24, 2006.
Physical Therapist • The physical therapist is board certified orthopaedic specialist (OCS, 1995), by the American Board of Physical Therapy Specialties (ABPTS), a fellow of the American Academy of Orthopaedic Manual Physical Therapy (FAAOMPT, 1997) and in private practice. He has 25 years of experience in orthopaedic physical therapy.
Demographics • 2006: Prospective (n=26), mean age=56.5 (±16.5) • Men: n=11 (mean age= 61 (±16.6)) • Women: n=14 (mean age=53.8 (±15.34)) • 2001 Retrospective (n=28), mean age= 47.7 (±16.7) • Men: n=13(mean age=44 (±14.2) • Women: n=15 (mean age= 50.9 (±18.6)
Acute/Subacute LBP • 2006: Prospective (n=13) mean age=61 (±12.2) • Men (n=7) mean age=66.7 (±5.06) • Women (n=6) mean age=49.9 (±20.5) • Mean # Rx=4.2 (±2.01) • 2001: Retrospective (n=10) mean age=45.8 (±15.01) • Men (n=4) mean age=43 (±11.03) • Women (n=6) mean age=43.1 (±19.85) • Mean # Rx=6.2 (±3.2)
Chronic LBP • Prospective (n=13) mean age=52.7 (±17.5) • Men (n=4) mean age=51 (±25.5) • Women (n=9) mean age=53.4 (±15.8) • Mean # Rx= 5.08 (±4.2) • Retrospective (n=18) mean age=48.5 (±17.6) • Men (n=9) mean age=44.2 (±15.95) • Women (n=9) mean age=53.33 (±18.8) • Mean # Rx=6.93 (±4.16)
Patients with Acute LBP Rx=6.2 visits Rx=4.2 visits
Change in Oswestry per Rx • Change in Oswestry score per treatment: • 2001 Retrospective: 7.2 pt change/ 6.2 Rx= 1.2 pts/ Rx • 2006 Prospective: 15.9 pt change/ 4.2 Rx = 3.8 pts/ Rx 3x Oswestry score improvement per 2006 Rx vs. 2001 Rx! Rx=6.2 visits Osw MCID >6 Rx=4.2 visits
Patients with Acute LBP • Change in NPRS per treatment • 2001 Retrospective: 1.6 pt change/ 6.2 Rx= 0.26 pts/ Rx • 2006 Prospective: 3.2 pt change/ 4.2 Rx = 0.76 pts/ Rx 3x the NPRS Improvement per 2006 Rx vs. 2001 Rx! NPRS MCID > 2.0 pts
Acute LBP: First 4 Weeks of Care • Net change • 2006: • 7.2 Osw pts @ 2 wks • 13.7 Osw pts @ 4 wks • 2001: • (-) 5.4 Osw pts in 2 wks • 5.4 Osw pts in 4 wks • Percentage change • 2006: • 20.2 % @ 2 wks • 38.7% @ 4 wks • 2001: • (-) 15.6% @ 2 wks • 15.6% @ 4 wks
Acute LBP: First 4 Weeks of Care • Net change • 2006: • 2.0 pts in 2 wks • 2.9 pts in 4 wks • 2001: • 0 pts in 2 wks • 1.5 pts in 4 wks • Percentage change • 2006: • 20% in 2 wks • 54.7% in 4 wks • 2001: • 0% in 2 wks • 31.3% in 4 wks
Patients with Chronic LBP Rx= 5.1 visits Rx=6.9 visits
Patients with Chronic LBP • Change of Oswestry score points/ # Rx • Prospective (2006): 9.9/5.1 visits: 1.9 pts / Rx • Retrospective (2001): 16.3/6.9 Rx= 2.4 pts/ Rx 2001: Oswestry score 0.5 point Per treatment better over 2006… not a clinically significant difference. Rx= 5.1 visits Rx=6.9 visits
Patients with Chronic LBP • Change of NPRS score points/ # Rx • Prospective (2006): 1.8 pts/ 5.1 Rx: 0.35 pts / Rx • Retrospective (2001): 1.0 pts/ 6.9 Rx= 0.15 pts/ Rx 2006: Chronic LBP had 2x The improvement per Rx vs. 2001 for pain (NPRS).