Download
1 / 40
400 likes | 495 Views
Domestic Violence Medical Response Bridging the gap between Medical Forensics Law Enforcement and Advocacy Nancy O’Malley District Attorney Alameda County Hillary Larkin, PA-C, SART/ DV Clinical Director Alameda County Medical Center. Bridging GAPS Advocacy and Law Enforcement.

E N D
Domestic Violence Medical ResponseBridging the gap betweenMedical ForensicsLaw EnforcementandAdvocacyNancy O’Malley District Attorney Alameda CountyHillary Larkin, PA-C, SART/ DV Clinical DirectorAlameda County Medical Center
Bridging GAPSAdvocacy and Law Enforcement • Learning from our Success • ACFJC opens • Increase in Victim’s participating in prosecution
DV cases not filed by DA due to “victim refusing to cooperate” ACFJC working together for change Factors that effect victim’s decision to cooperate time between assault and investigation/charges -Lack of confidence in the system -Lack of resources available for the victim if they decide to testify against the batterer
After DA’s DV unit moves to ACFJC ACFJC working together for change • More victims are decide to cooperate with prosecution • The number of felony DV cases increased from 37% (2005) to 58% (2008) • The number of DV cases filed as a felony (as opposed to misdemeanor) increase from 13% (2005) to 20% (2008) • shorten time between assault and investigation • building confidence in the system • providing resources to enable victims to testify against batterer
DV cases not charged because “the victim declined cooperation” ACFJC working together for change
Bridging GapsAdvocacy and Medical • SART teams • IPV forensic teams
Interdisciplinary DV response in a health care setting ACFJC working together for change • Key Elements Inquiry and referral Onsite resources Leadership and Quality Improvement Community linkage (ACFJC) Supportive Environment
Supportive Environment ACFJC working together for change • Information available: restrooms, exam rooms, online outreach to pts, podcasts, health ed classes • Posters: “Let us know, we can help” • Reaching patients anywhere they contact the health system • Engaged and informed workforce DV poster
Inquiry and referral ACFJC working together for change • Role of the Health care provider is clear and limited • ASK • AFFIRM • ASSESS • DOCUMENT (report) • REFER
Onsite IPV response ACFJC working together for change • Options • on-site advocacy from local agency • on-call advocate to the hospital • in-house DV trained Social service/mental health staff • brief intervention • private place to access help via phone or on-line
Community Linkage • Family Justice Center • Co- located services for DV
Medical- Advocacy Tasks ACFJC working together for change • Danger Assessment • Safety Plan • Emergency Shelter/transitional housing • Plan for medical/ mental health follow up • Warm hand off to the FJC
DV services must support nationalHealthCare priorities ACFJC working together for change • Patient centered • safe effective, efficient care • evidence informed • reduce health care disparities • prevent injury and chronic disease • improve population health and wellness
IOMinstitute of medicine ACFJC working together for change • July 2011 • Recommends that preventive Services for women be covered as part of the Patient Protection and Affordable Care Act 2010 • including • screening for cervical cancer, STI, hiv screening • contraceptive education, counseling, methods and services • prenatal screening and lactation counseling for pregnant women • well-woman annual health screening • screening and counseling for all woman and adolescent girls for IPV and DV in a culturally sensitive and supportive manner
ACOG(Feb 2012) • “Based on the prevalence and health burden of IPV among women, education about IPV; screening at periodic intervals, including during obstetric visits; and ongoing clinical care can improve the lives of women who experience IPV. Preventing the lifelong consequences associated with IPV can have a positive effect on the reproductive, perinatal, and overall health of all women.”
JCAHO • PC.01.02.09 and PC.3.10 (behavioral health) • Hospital Assesses the pt who maybe a victim of abuse • Assist in referrals • educates staff to recognize victims and potential victims • Screening for DV when entering system • Reports abuse to external agencies in accordance with the laws and regulation • Standard R1.01.06.03 • Protects pt from abuse while in the hospital, receiving care • Evaluates allegations, observations and suspected cases of abuse that occur in the hospital. Reports to appropriate authorities
State laws and mandatory reporting • Are you familiar with you state’s laws • that govern health care reporting of injuries, suspected abuse and or DV to police? • requiring health care protocols, screening for DV, or training for HCPs?
States laws mandating HCPsprotocols, screening, training • very few states have enacted statutes requiring DV health care protocols, or screening requirements for HCP/ facilities • 15 states have laws requiring training on DV for HCP. • Reference: • Compendium of State Statutes and policies on Domestic Violence and Health Care, produced by the Family Violence Prevention Fund
Mandatory Reporting of Injuries • 47 states and DC have enacted mandatory reporting legislation. • 3 categories- Require report of injuries • caused by a weapon (stab, GSW) • sustained in violation of criminal laws, as result of violence, or through non accidental means • sustained in DV
Bridging Gap betweenMedical And Law enforcement • Reporting to Law enforcement • Balance protection of patients rights and holding batterers accountable • Providing forensically meaningful information • Requires advocacy to be educated/ non-biased/
Report Requirements( Calif Penal Code 11160-11163.6) • The law requires that any health care practitioner employed in a health facility, who in a professional capacity, within the scope of their employment, who has knowledge of, or observes a patient, who is known to or reasonably suspects, has suffered a wound or physical injury as a result of assaultive or abusive conduct, must report to law enforcement
Report Requirements( Calif Penal Code 11160-11163.6) • Who is included in the definition of DV • current or past intimate partners • individuals with children in common • adult family members or individuals that share a home • What information is included • name and whereabouts of the victim • location and time of the assault • nature of the injuries • Name of the suspected or reported perpetrator
Making the Mandatory Report to LE • Inform the patient of the clinician’s duty to report • Inform the pt of likely response from LE • Make telephone report • Complete documentation- providing all information required by law • Include special instructions for safety- Maximize pt input (advocacy can help) • Copy sent to LE, to Medical record and kept CONFIDENTIAL (sequestered files) only accessible by consent of the patient
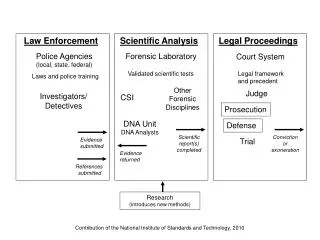
Bridging the gap between medical and law enforcement • documenting medical injuries in a meaningful way • providing medically relevant reports for LE is different then disclosing a entire medical record • Medical examiners are unbiased observers - different from advocates
Creating a medically relevant chart • Ask history questions based on what we know about the danger assessment • Use a body map to help non medical personnel understand the type and severity of injury • Document inconsistencies and in hx and physical findings
Trauma informedServices • incorporate knowledge about trauma-prevalence, impact, and recovery- in all aspects of service delivery • minimize re-victimization • facilitate recovery and empowerment • Psychological Trauma • Refers to the individual’s perception of significant events or circumstances, past or present. These events may result in a cluster of symptoms, adaptations, and reactions that interfere with the individuals functioning. “ Healing happens in relationships”
Trauma Informed Services • Based on the Adverse Childhood Experiences (ACE) Study (Felitti) • those experiencing ACE’s are at higher risk for chronic health problems, substance abuse, depression/SI, accidental or non accidental injury. • Changes are neurological, biological, psychological, and social in nature.
Strangulation • “ a form of asphyxia characterized by closure of the blood vessels or air passages of the neck as a result of external pressure on the neck.” • Iserson K, Strangulation: a review of ligature, manual and postural compression injuries. Annotated Emerg Med 1984; 13(3); 179-85 • Mitchell C, Intimate Partner Violence: A Heath-Based Perspective 2009
DVRR • Domestic Violence Reporting and Referral • Pilot project for the Alameda County Medical Center and the Alameda County FJC • Funded through a grant from Verizon