Download
1 / 24
260 likes | 450 Views
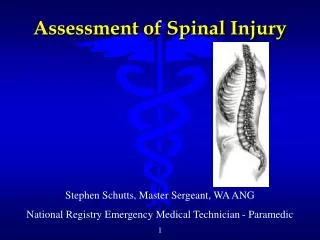
Emergency Spinal Radiological Assessment. spine injury: location. C. type neurologic sequelae 1. cervical . . . . . . brainstem, cord or root 2. thoracic . . . . . cord or root 3. lumbar . . . . . . conus or root. T. L. cord injury: deficit patterns.

E N D
spine injury: location C typeneurologic sequelae 1. cervical . . . . . . brainstem, cord or root 2. thoracic . . . . . cord or root 3. lumbar . . . . . . conus or root T L
cord injury: deficit patterns 1. normal (no neurologic injury) 2. incomplete deficit (syndromes) a. central cord b. anterior cord c. Brown-Sequard d. posterior cord e. conus/epiconus 3. complete functional transection
spine injury: types • muscular/ligamentous • a. contusions • b. strains • c. sprains • d. complete ligamentous disruption • 2. fractures + / - dislocation stability: 1. stable 2. unstable
spinal Imaging after trauma - indications • clinical indications • a. spine-region pain • b. neurologic deficit • (1) radicular • (2) cord • c. severe multisystem injuries • d. altered mental status • clinical rationale • a. prevent cord, root injury (neurologic stability) • b. prevent incapacitating deformity and pain (mechanical instability)
Which patients need imaging of the cervical spine? no imaging needed Case 1: mild/moderate trauma patient • no loss of consciousness • normal mental status (and not intoxicated) • no neck pain or tenderness • no neurologic deficit
Which patients need imaging of the cervical spine? Case 2: mild/moderate trauma patient • altered mental status (patient is obtunded and/or intoxicated) • neck pain or tenderness • neurologic symptoms or deficit
Which patients need imaging of the cervical spine? imaging needed Case 3: severe multi-system trauma patient
spinal Imaging after trauma – imaging tools • bony - fractures/dislocations • a. X-rays – AP, lateral, open-mouth odontoid • b. CT scan • ligamentous • a. MRI scan • b. flexion – extension lateral x-ray • 3. disk injury • a. MRI scan • b. CT/myelogram
cervical: 7 • lordotic curve • thoracic: 12 • kyphotic curve • lumbar: 5 • lordotic curve
spine injury: alignment 1. pre-vertebral fascia 2. anterior marginal line 3. posterior marginal line 4. spino-laminar line 5. posterior spinous line 1 2 3 4 5 A. vertebral body width B. spinal canal diameter
ligamentous injury without fracture instability possible even with normal CT; early MRI helpful stabilize until neck pain resolves, assess competence of ligaments with flexion/extension X-rays or MRI
Bilateral facet fracture/dislocation: “jumped” or locked facets
C1 - Jefferson fracture axial loading often associated with C2 fractures assess transverse ligament
C2 - odontoid fractures/subluxations type I type II type III
C2 - Hangman’s fracture hyperextension/axial loading bilateral C2 pars interarticularis fracture unstable when: a. >3.5 mm subluxation of C2 on C3 b. >11 degrees angulation
Atlantoaxial subluxation • Atlantodental interval (ADI) • Left: Normal ADI ≤ 3 mm • Right: C1-2 subluxation
Denis 3-column model - thoracolumbar spine one-column injury usually stable two-column injury usually unstable three-column injury unstable
Class A: vertebral body compression compression fracture Anterior column failure Middle and posterior columns intact Unstable if >50% compression or >20 degrees angulation burst fracture Anterior and middle column failure Retropulsion of bone into canal Often have neurologic deficit Unstable
Class B: distraction (+ flexion/extension) Types Flexion/distraction (Chance, seat belt injury) Hyperextension Three-column injury: unstable
flexion/distraction posterior ligamentous injury
Class C: three-column injury with rotation fracture-dislocation shear injury unstable neurologic deficit