Download
1 / 35
570 likes | 1.82k Views
Assessment of cardiovascular system. Presented by Aisha Parveen. Objectives:. By the end of this presentation students will be able to: Review the Anatomy and Physiology of the cardiovascular system

E N D
Assessment of cardiovascular system Presented by Aisha Parveen
Objectives: By the end of this presentation students will be able to: • Review the Anatomy and Physiology of the cardiovascular system • Describe the components of health history that should be elicited during the assessment of cardiovascular system. • Identify the landmarks of the chest.
Objectives cont,…. Describe the following: • Pulse rate, rhythm and pulsation characteristics • PMI • Heart sounds • Discuss systolic and diastolic murmurs. • Assess the cardiovascular system systematically. • Document findings • List the changes in cardiovascular system that is characteristics of aging process.
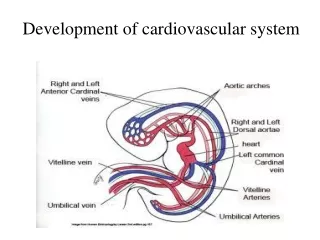
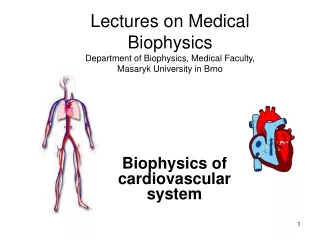
Anatomy and Physiology: • Heart and great vessels • Layers of the heart • Cardiac chambers and Valves • Conduction system of heart • Arterial pulses and blood pressure
Preparation for Assessment: • Room that is warm & “quiet” • Examining table positioned so you can stand on the patient’s right side • Patient should rest supine with the upper body elevated 30 to 45 degrees • Patient wearing gown • A watch with a second hand • Stethoscope with diaphragm & bell
Health History • Age • Gender • Obesity • Smoking and tobacco • Use of oral contraceptives • Hyperlipidemia • Hypertension • Diabetes • Assessment of sign and symptoms
Chest pain Site and radiation Character Severity Frequency Duration Aggravating factors Relieving factors Associated features Dysponea Onset Severity Related to effort Orthopnoea Paroxysmal nocturnal dyspnoea Edema Palpitations Health History
Other aspects of history • Past medical history • Drug history • Family history • Social history • Occupational history
Techniques of Examination: • The Arterial pulses: • Heart Rate • Rhythm • Quality or Amplitude • Blood Pressure: • Pressure exerted on the walls of the arteries during ventricular systole and diastole. • Range 100/60 mm Hg to 140/90 mm Hg • Average Normal BP is 120/80 mm Hg
Inspection • Posture • Signs of distress • Breathlessness • Skeletal abnormalities • Scars • Pulsations • Pacemaker • Cyanosis
Palpation • Check pulses for rate, rhythm and quality • Check for variation between location • Palpate for edema CardioVascular, 2009
Vascular Insufficiency CardioVascular, 2009
Palpation • PMI • Palpate using 1 finger • Midclavicular line, 5th intercostal space
Palpation Palpate: heaves and thrills CardioVascular, 2009
Percussion • Start well to the left on chest from resonance towards cardiac dullness in the 3rd, 4th & 5th intercostal space
Auscultation CardioVascular, 2009
Cardiac Sounds • S1 (lup) • Closure of AV valve • Beginning of systole • Louder at apex • S2 (dub) • Closure of semilunar valve • End of systole • Louder at base
Cardiac Sounds • S3 • Normal in young healthy • Impaired LV function • Raised end diastolic pressure • Low pitched at apex – bell • “gallop” or “triple” rhythm when tachycardic • S4 • Accompanies and is due to atrial systole • Only heard in sinus rhythm • Loud in left atrial hypertrophy i.e. IHD, hypertension • Low pitched at apex – bell
Cardiac Sounds • Murmurs • Differentiated from heart sounds by longer duration • Turbulent flow across valves • Leaking or narrowed valve • Timing • Intensity CardioVascular, 2009
Assessment of the Jugular Vein: • Purpose: To measure the “central venous pressure” • Method: Position patient @ 45 degree angle at the hip Turn head slightly away Use a strong light tangentially Observe the external jugular over the sternomastoid muscle
Jugular Venous Pressure 30 CardioVascular, 2009
CVS Changes with Aging • Stiffer, less compliant arterial tree • Increased vascular resistance and impedance • Prolonged cardiac relaxation and contraction • Incompetent chronotropic and inotropic CardioVascular, 2009
CVS Changes with Aging • Incompetent valves of the veins • Less sensitive baroreceptors • Heart muscle loses elasticity • Decrease hematocrit CardioVascular, 2009
Heart valves become thickened by fibrosis and more rigid (leading to murmurs) • Pacemaker cells decreases • Conduction pathway become less efficient CardioVascular, 2009
Reference Bickley, L.S., & Szilagyi, P.G. (2003). Bates’ Guide to: Physical Examination and History Taking. (ed. 7th). Lippincott: Philadelphia. Ellen, E.M. (1998). Helath Assessment and Physical Examination. DelmarPublishers: Albany, N.Y. CardioVascular, 2009