Download
1 / 16

E N D
Never say No, never say, ‘I cannot’, for you are infinite. Even time and space are as nothing compared with your nature. You can do anything and everything. -- Swami Vivekananda
Shashidhar Venkatesh Murthy A/Prof & Head of Pathology College of Medicine & Dentistry ….. foundation of clinical medicine Clinical Pathology: RBC 1.3: Hemolytic Anemia - Acquired CPC System Topic : Term2 Week1 - Haem 1/2. : Haematology - RBC Disorders. : 1: Anemia Intro 2: IDA, MBA & ACD 3: Acquired HA 4: Congenital HA. 5: Others.
Pathogenetic Classification of Anemia: Top 6 Anemias: 1. Iron Def. A 2. Megaloblastic 3. Anem. Of Chronic Dis. 4. Aplastic An. 5. Immune Hemolytic – Warm 6. Immune Hemolytic - Cold Decreased Production: Nutrient Deficiency. Iron def (IDA) / Megaloblastic (MBA) Hemopoietic cell defect: Anemia of chronic disorders (ACD) Aplastic anemia (AA). Dysplastic anemia. Myelodysplastic Syndromes Increased loss / destruction: Blood loss anemia – Acute / Chronic - bleeding. Hemolytic anemia – Congenital / Acquired. Acquired / External injury. Immune AIHA (Warm/Cold) Mechanical, Drugs & Parasites Congenital / Internal RBC defect Defective Membrane (Spherocytic an) Defective Hemoglobin (Sickle cell an.) Deficient Enzyme (G6PD) 2 3
1. Pallor Haemolytic Anemia: Introduction Anemia due to Increased RBC destruction life span (<120d) - Abnormal forms Bilirubin Jaundice (Unconjugated) RBC production – BM Hyperplasia & Reticulocytes. Acute: Pallor, Jaundice (normal urine) Chronic: Splenomegaly, pigment gall stones. Intravascular & Extravascular Hemolysis*. 2. Jaundice Jaundice 3. Pigment Gall stones Globins Iron Immune Mech. Infection Conjugation Bil. Conj Normal Porphyrin Bil. Unconj 4. Splenomegaly
Intravascular Hemolysis. Breakdown of RBC within Blood Vessel Etiology: Immune, Mechanical, Enzyme def. transfusion mismatch, drugs, infections. Lab diagnosis: Absent Haptoglobins. Haemoglobinemia Haemoglobinuria Haemosiderinuria Clinical features: Shock, Renal failure, Renal failure In Extravascular Hemolysis: Unconjugated hyperbilirubinemia only* 5
Hemolytic anemia: Morphology Abnormal RBC shapes spherocytes in WIHA, target forms in thalasssemia etc. Polychromatophils. (Immature RBC - large, bluish, no central palor - Reticulocytes) Nucleated RBC small nucleus inside reticulocyte. Giems stain (routine blood film) Bluish, Large RBC ( MCV) Warm Ab Hemolytic Anemia Thalassemia 7
Hemolytic Anemia: Reticulocytes Methylene blue stain for cytoplasmic RNA Reticulocyte RBC Giemsa stain (routine blood film) Bluish, Large RBC ( MCV) Reticulocytosis Increased RBC production
Only educated person is one who has learned how to learn and change. -- Carl Rogers
Haemolytic Anemia: classification Acquired / External Injury: Immune: IgG / Warm & IgM / Cold Physical: valve dis, March Hb.nuria, trauma, burns. Drugs: α-Methyldopa, cephalosporins, ibuprofen etc. Parasites / infections (malaria, septicemia (DIC) Congenital / Internal defects: Defective Membrane: Spherocytic anemia. Defective Haemoglobin: Sickle cell anemia, Thalassemia Deficient Enzyme: G6PD deficiency anemia. Cell Mem Hb Enzymes 10
Immune Hemolytic anemia IgG/IgM: Causes: RBC Antibody (Commonest.) Pathogenesis: Warm / IgG coated RBC lysis in spleen. Drugs, Idiopathic. (predominantly extravascular) Cold / IgM - (Infections, Lymphoma) RBC Clumping & complement fixation lysis in BV & Liver. (predominantly intravascular) Morphology: Spherocytes (warm) / RBC clumps (cold). Clinical Features: Anemia, Jaundice. Splenomegaly in chronic. Diagnosis: Comb’s test *. IgG IgM IgG Antibody COLD WARM WARM / IgG COLD / IgM 11
AIHA: Lab diagnosis – Coombs test. Patient RBC Patient Serum Direct Coombs Test: (for antigen on patient RBC) Indirect Coombs Test: (for antibodies in the serum.) Pos Neg Online Video Tutorial 12
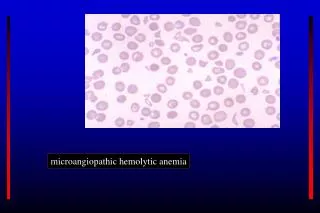
MAHA - Microangiopathic Hemolytic An. Mechanical damage: Etiology: DIC, TTP, HUS Valve disease / Artificial valves. March Hemoglobinuria. Morphology: Fragmented RBC: Schistocytes. Polychromasia – reticulocytes. 13
The only person who never makes a mistake is a person who never does anything…! - Theodore Roosevelt 14
You are the stone.. Need help? contact me… 1. Office location: DB39-136 (Townsville) 2. Office Tel: 4781 4566 3. Email: venkatesh.shashidhar@jcu.edu.au 4. Emergency?: 0416933704 Need personal coaching? Email me for an appointment.
The pessimist waits for better times, and expects to keep on waiting; the optimist goes to work with the best that is at hand now, and proceeds to create better times. -- Christian D. Larson