Download
1 / 45
450 likes | 459 Views
Explore the composition, characteristics, and functions of blood, including hematopoiesis, RBC production, and the role of blood in transportation, regulation, and protection.

E N D
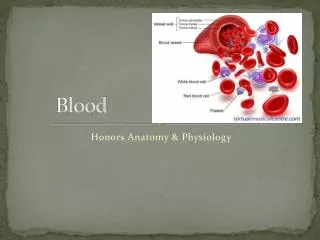
Blood Exercise 29
Fluids of Body The cells of the body are serviced by 2 fluids • Blood • Interstitial fluid Hematologyis study of blood and blood disorders
Major Body Fluids I. Blood • composed of plasma and a variety of cells • transports nutrients and wastes II. Interstitial fluid • Found within tissues • Bathes and surrounds the cells Nutrients and oxygen diffuse from the blood into the interstitial fluid & then into the cells Wastes move in the reverse direction
Functions of Blood 1. Transportation • O2, CO2, metabolic wastes, nutrients, heat & hormones 2. Regulation • helps regulate pH through buffers • helps regulate body temperature - coolant properties of water - vasodilatation of surface vessels dump heat/ vasocontriction conserves heat • helps regulate water content of cells by interactions with dissolved ions and proteins 3. Protection from disease & loss of blood
Physical Characteristics of Blood • Thicker (more viscous) than water and flows more slowly than water • Temperature of 100.4 degrees F • pH 7.4 (7.35-7.45) • 8 % of total body weight Blood volume • 5 to 6 liters in average male • 4 to 5 liters in average female • hormonal negative feedback systems maintain constant blood volume and osmotic pressure
Techniques of Blood Sampling Venipuncture • sample taken from vein with hypodermic needle & syringe • median cubital vein • less pressure • closer to the surface Finger or heel stick • common technique for diabetics to monitor daily blood sugar • method used for infants Why not stick an artery? When do we use an artery?
Composition of Whole Blood • 55% plasma • 45% cells - 99% RBCs - < 1% WBCs and platelets
Plasma Over 90% water 7% plasma proteins -created in liver; confined to bloodstream 1. albumin - maintains blood osmotic pressure 2. globulins (Immunoglobulins) - antibodies bind to foreign substances called antigens; form antigen-antibody complexes 3.fibrinogen - for clotting 3 % other substances - electrolytes, nutrients, hormones, gases, waste products
Formed Elements 1. Red blood cells ( erythrocytes ) 2. White blood cells ( leukocytes ) • granular leukocytes – neutrophils, eosinophils, basophils • agranular leukocytes – lymphocytes ( T cells, B cells, and natural killer cells), monocytes 3. Platelets (special cell fragments)
Hematocrit • Percentage of blood occupied by cells female normal range - 38 - 46% (average of 42%) male normal range - 40 - 54% (average of 46%) testosterone’s role • Anemia - not enough RBCs or not enough hemoglobin • Polycythemia - too many RBCs (over 65%); dehydration, tissue hypoxia, blood doping in athletes
Blood Doping • Injecting previously stored RBC’s before an athletic event; more cells available to deliver oxygen to tissues • Dangerous - increases blood viscosity; forces heart to work harder
Formation of Blood Cells • Most blood cells types need to be continually replaced die within hours, days or weeks • Process of blood cells formation is hematopoiesis or hemopoiesis • In the embryo - occurs in yolk sac, liver, spleen, thymus, lymph nodes & red bone marrow • In adult - occurs only in red marrow of flat bones like sternum, ribs, skull & pelvis and ends of long bones
Hemopoietic Growth Factors • Regulate differentiation & proliferation • Erythropoietin (EPO) - produced by the kidneys increase RBC precursors • Thrombopoietin (TPO) - hormone from liver stimulates platelet formation • Cytokines are local hormones of bone marrow - produced by some marrow cells to stimulate proliferation in other marrow cells; colony-stimulating factor (CSF) & interleukin stimulate WBC production
Erythrocyte or red blood cell • Contain oxygen-carrying protein hemoglobin that gives blood its red color • 1/3 of cell’s weight is hemoglobin • Biconcave disk 8 microns in diameter • increased surface area/volume ratio • flexible shape for narrow passages • no nucleus or other organelles • no cell division or mitochondrial ATP formation
Normal RBC count • male 5.4 million/drop ---- female 4.8 million/drop • new RBCs enter circulation at 2 million/second
Erythrocyte Life Cycle • RBCs live only 120 days • wear out from bending to fit through capillaries • no repair possible due to lack of organelles • Worn out cells removed by fixed macrophages in spleen & liver
Erythropoiesis: Production of RBCs • Proerythroblast starts to produce hemoglobin • Many steps later, nucleus is ejected & a reticulocyte is formed • orange in color with traces of visible rough ER • Reticulocytes escape from bone marrow into the blood • In 1-2 days, they eject the remaining organelles to become a mature RBC
Feedback Control of RBC Production Tissue hypoxia (cells not getting enough O2) • high altitude since air has less O2 • anemia RBC production falls below RBC destruction • circulatory problems • Kidney response to hypoxiarelease erythropoietinspeeds up development of proerythroblasts into reticulocytes
WBC Anatomy and Types • All WBCs (leukocytes) have a nucleus and no hemoglobin • Granular or agranular classification based on presence of cytoplasmic granules made visible by staining • granulocytes are neutrophils, eosinophils or basophils • agranulocytes are monocyes or lymphocytes
Neutrophils (Granulocyte) • Polymorphonuclear Leukocytes or Polys • Nuclei = 2 to 5 lobes connected by thin strands • older cells have more lobes • Fine, pale lilac practically invisible granules • 60 to 70% of circulating WBCs
Neutrophil Function • Fastest response of all WBC to bacteria • Direct actions against bacteria • release lysozymes which destroy/digest bacteria • release defensin proteins that act like antibiotics • release strong oxidants (bleach-like, strong chemicals ) that destroy bacteria
Basophils (Granulocyte) • Large, dark purple, variable-sized granules stain with basic dyes • Irregular, s-shaped, bilobed nuclei • Less than 1% of circulating WBCs
Basophil Function • Involved in inflammatory and allergy reactions • Leave capillaries & enter connective tissue as mast cells • Release heparin, histamine & serotonin • heighten the inflammatory response and account for hypersensitivity (allergic) reaction
Eosinophils (Granulocyte) • Nucleus with 2 or 3 lobes connected by a thin strand • Large, uniform-sized granules stain orange-red with acidic dyes • 2 to 4% of circulating WBCs
Eosinophil Function • Leave capillaries to enter tissue fluid • Attack parasitic worms • Phagocytize antibody-antigen complexes
Lymphocyte (Agranulocyte) • Dark, oval to round nucleus • Cytoplasm sky blue in color • amount varies from rim of blue to normal amount • increase in number during viral infections • 20 to 25% of circulating WBCs
Lymphocyte Functions • destroy bacteria and their toxins; turn into plasma cells that produces antibodies • attack viruses, fungi, transplanted organs, cancer cells & some bacteria • attack many different microbes & some tumor cells; destroy foreign invaders by direct attack
Monocyte (Agranulocyte) Largest WBC in circulating blood • does not remain in blood long before migrating to the tissues; differentiate into macrophages fixed group found in specific tissues • alveolar macrophages in lungs • kupffer cells in liver • wandering group gathers at sites of infection • Cytoplasm is a foamy blue-gray ; kidney shaped nucleus; 3 to 8% of circulating WBCs;
Monocyte Function • Take longer to get to site of infection, but arrive in larger numbers • Become wandering macrophages, once they leave the capillaries • Destroy microbes and clean up dead tissue following an infection
WBC Physiology • Less numerous than RBCs • 5000 to 10,000 cells per drop of blood • Leukocytosis is a high white blood cell count - microbes, strenuous exercise, anesthesia or surgery • Leukopenia is low white blood cell count - radiation, shock or chemotherapy • Only 2% of total WBC population is in circulating blood at any given time • rest is in lymphatic fluid, skin, lungs, lymph nodes & spleen
Differential White Blood Count • Detection of changes in numbers of circulating WBCs (percentages of each type) - indicates infection, poisoning, leukemia, chemotherapy, parasites or allergy reaction • Normal WBC counts • neutrophils 60-70% (up if bacterial infection) • lymphocyte 20-25% (up if viral infection) • monocytes 3 -- 8 % (up if fungal/viral infection) • eosinophil 2 -- 4 % (up if parasite or allergy reaction) • basophil <1% (up if allergy reaction or hypothyroid)
Platelet (Thrombocyte) Anatomy • Disc-shaped, 2 - 4 micron cell fragment with no nucleus • Normal platelet count is 150,000-400,000/drop of blood • Other blood cell counts • 5 million red & 5-10,000 white blood cells
Platelets--Life History • Platelets form in bone marrow: Short life span (5 to 9 days in bloodstream) • formed in bone marrow • few days in circulating blood • aged ones removed by fixed macrophages in liver and spleen
Complete Blood Count • Screens for anemia and infection • Total RBC, WBC & platelet counts; differential WBC; hematocrit and hemoglobin measurements Normal hemoglobin range • infants have 14 to 20 g/100mL of blood • adult females have 12 to 16 g/100mL of blood • adult males have 13.5 to 18g/100mL of blood
BLOOD TRANSFUSIONS • If a type A person is given type A cells, the A cells will be accepted. • If a type A person is given type O cells, the O cells will be accepted. • If a type A person is given type B cells, the B cells will be destroyed. • If a type A person is given type AB cells, the AB cells will be destroyed. • Which blood types can O accept? • Which blood types can O donate to?
Rh factor • Many people also have a so called Rh factor on the red blood cell's surface. This is also an antigen and those who have it are called Rh+. Those who haven't are called Rh-. A person with Rh- blood does not have Rh antibodies naturally in the blood plasma (as one can have A or B antibodies, for instance). But a person with Rh- blood can develop Rh antibodies in the blood plasma if he or she receives blood from a person with Rh+ blood, whose Rh antigens can trigger the production of Rh antibodies. A person with Rh+ blood can receive blood from a person with Rh- blood without a reaction.
Rh Factor and Pregnancy of Rh Negative Mother 1st baby = Rh + Mother makes antibodies to Rh at birth 2nd baby = Rh - No problems. Nothing for mother’s antibodies to attack. 3rd baby = Rh + Mother’s antibodies will cross placenta during pregnancy and attack baby’s RBCs. Erythroblastosis fetalis