Download
1 / 23
230 likes | 356 Views
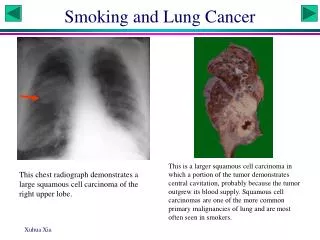
Smoking in Chronic Lung Disease. Karl Fagerström, Ph.D. Smokers Information Centre, Helsingborg, Sweden. REDUCE RISK FACTORS IN COPD: KEY POINTS.

E N D
Smoking in Chronic Lung Disease Karl Fagerström, Ph.D. Smokers Information Centre, Helsingborg, Sweden
REDUCE RISK FACTORSIN COPD: KEY POINTS • Reduction of total personal exposure to tobacco smoke, occupational dusts and chemicals, and indoor and outdoor air pollutants are important goals to prevent the onset and progression of COPD. • Smoking cessation is the single most effective-and cost-effective- intervention to reduce the risk of developing COPD and stop its progression (Evidence A).
Smoking Cessation and Respiratory Symptoms • AmerStudy: 5887 ADULT SMOKERS WITH EARLY COPD FOLLOWED UP FOR 5 YEARS • 2/3 UNDERWENT SMOKING INTERVENTIONS; 1/3 USUAL CARE • SMOKING CESSATION IN 22% vs 5% • LESS PREVALENCE OF CHRONIC COUGH, CHRONIC PHLEGM, WHEEZING AND SHORTNESS OF BREATH (p<0.0001) • RESPIRATORY SYMPTOMS ASSOCIATED WITH GREATER LOSS IN FEV1 (p<0.001) • . Lung (Kanner RE et al., Am J Med 1999)
Smoking Cessation & Lung Function • 5887 ADULT SMOKERS WITH EARLY COPD FOLLOWED UP FOR 5 YEARS • MEAN ANNUAL RATE OF LOSS IN FEV1: • QUITTERS (1st y.) -0.33% (+/-0.05) • INTERMITTENT SM. -0.58% (+/-0.05) • SMOKERS -1.18% (+/-0.03) Murray, Anthonisen et al. J.Clin Epidem. 1998
SMOKING CESSATION DECREASES MORTALITY American Lung Health Study At 14,5 years follow up The group randomized to smoking cessation had significantly less all cause mortality, OR 1,18 (1,02-1,37) Anthonisen et al Ann Intern Med 2005
COPD - Reasons to smoke: Avoid strong withdrawal symptoms Treat cognitive deficits Control depression Help clearing the airways
Smokers with high dependence, depression or COPD have less success in breaking the tobacco dependence Tönnesen 1986
SMOKERS COPD N=153 HEALTHY N=870 DEPENDENCE 4.8 3.1 p<.001 (FTND) CARB. MONOX. 19.7 ppm 15.4 ppm p<.000 Jimenéz-Ruiz et al. 2001
CARBON MONOXIDE CAN BE USED TO: • Indicate smoke intake • Indicate dependence • Increase motivation to give up • Monitor progress when quitting • and reducing smoking
Carbon Monoxide: Approximate cut offs. Non-Smokers 1-3 ppm Average Smokers 10-20 ppm Heavy Smokers 21-70 ppm
PHARMACOTHERAPY • NICOTINE REPLACEMENT • BUPROPION • (NORTRYPTILENE)
Assumptions in nicotine intake 1 cigarette 1,5 mg 2 mg gum 1,2 4 mg gum 2,8 21 mg patch 21 15 mg patch 15
Combining NR products has usually • yielded higher success rates. • Because of • Higher dose • A tool to deal with break-through cravings
USING NR BEFORE QUITTING Two studies used NR before quitting with increased results. Before quitting At qutting Herrera, Fagerström et al. 1995 61% 52%* Schuurmans, Bolliger et al 2004 22% 12% Rose et al. 2006 15% 6%* * At six weeks
Many heavy smokers have bronchial Inflammation and obstruction Many relapse early to find relief from exacerbations Therefore preventive treatment has been tried 72 smokers, normal LF, randomized to NRT +beta2 stimulant NRT Smoke free 86% 47% Anotov, Sakharova 2006.
NRT NRT + β2 adrenergic stimulant Days Anotov, Sakharova 2006
What to do with those unable or unwilling to stop abruptly?
Do we serve more smokers by offering reduction? Two samples (N=106, N=236) from an HMO coming for outpatient surgery were offered advice to stop or reduce smoking. Selection Reduction by 2/3 Abrupt cess. Nothing Sample 1 39% 38% 23% Sample 2 22% 12% 65% Glasgow et al. 2006
How Much Smoking Reduction Is Needed for Harm Reduction to take place? 50% has gradually developed as a standard < 8 cigarettes per day? Clearly the less smoked the better
DAGNOSING THE SMOKERASSESSMENTS Motives and motivationfor quitting Amount smoked Dependence level Fagerstrom test / Nicotine / Cotinine Carbon monoxide in exhaled air Spirometry Earlier quitting experience Psychic comorbidity
Chinese Monkey Gives up Smoking After 16 Years The 27 year old monkey Ai Ai that has smoked for 16 years has given up. Ai Ais guard has successfully helped her give up with walks after breakfast, music after lunch and exercise after supper. “In the beginning Ai Ai had cravings for cigarettes but as her life became richer she was able to for- get the cigarettes” says the guard. The nicotine dependence began when Ai Ai suffered from lonli- ness and sorrow after two caretakers died. In 1989 in Safari Park “Shaanxi” she began to smoke as her first caretaker died. 1997 she became a chain-smoker when her second caretaker died and her daughter was transfered to another Zoo. Wherefrom the monkey got her first cigarette and how smoking was maintained is not told. The Zoo will now find a new caretaker for her. APA Oct. 3 2005