Download

1 / 20
200 likes | 487 Views
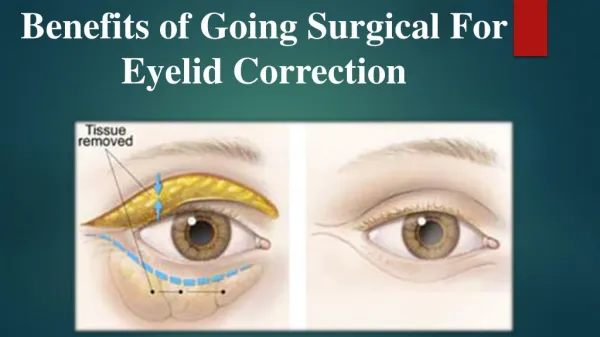
Vjacheslav Kuznetsov , Inga Borisikova Acu Mikrokirurgijas Centrs (Eye Microsurgery Centre) Riga, Latvia. Benefit of silicon-hydrogel contact lenses for patients undergoing combined surgical myopia correction. Contact lenses.

E N D
Vjacheslav Kuznetsov, Inga Borisikova Acu Mikrokirurgijas Centrs (Eye Microsurgery Centre) Riga, Latvia Benefit of silicon-hydrogel contact lenses for patients undergoing combined surgical myopia correction
Contact lenses • Patients are not always satisfied by the constant wear of contact lenses: • Hence the need for other options: • orthokeratology • surgery • Surgery helps patients who are unhappy with lenses. • Could lenses help those who are not satisfied after surgery?
Eye Microsurgery Centrewww.lazer.lv • a private ophthalmology clinic established in 1998 • the main activities of the Centre: • refractive surgery • surgical, therapeutic and laser treatment (cataract, glaucoma, retinal distrophy, etc) • we are one of very rare European clinics that offer all kinds of vision correction
Classification of vision correction We classify vision correction kinds according to their impact on the eye tissues: 1. Glasses – non-contact 2. Lenses – contact, but without permanent effect 3. Microsurgery – mechanical modification 4. Laser – excimer (ectomy) or coagulation 5. Implants – implantation of foreign bodies (corneal rings and intraocular lenses) 6. Radiofrequency – conductive keratoplasty Various combinations are possible
Myopia correction • Lenses - most frequent • Plus - cheap, easily available, non-traumatic • Minus - care necessary, foreign body • Excimer laser - most frequent surgery • Plus - technically simple, high precision • Minus - expensive, anatomical limitations, complications • Radial keratotomy - gradually loses popularity • Plus - least traumatic and anatomically most advantageous technique:optical centre remains intact • Minus - experience and high skill necessary Could combining the methods overcome their shortcomings?
Observation 1 • Our Centre has been performing radial keratotomies (RK) for 10 years, since 1998. • We saw that it is not always possible to achieve eumetropia, both for anatomical and technical reasons. • Additional keratotomy for better vision is possible after the cornea stabilizes. • But we found it easier to make adjustment, modifying the untouched central cornea by excimer laser, than to cut once more at the scarred peripheral cornea.
Observation 2 • We have been using excimer laser for 2 years. • We see that the effect of laser surgery depends on the corneal thickness and is additionally restricted by wide pupils and high astigmatism. • In case of thin cornea: • the achievement of good vision by excimer laser alone is doubtful • postoperative keratoconus becomes a problem • If the eye anatomy had been pretreated by radial keratotomy on the periphery, one needs to slice less of central cornea. • In this case the use of laser for thin corneas becomes possible and reasonable.
Benefits: • Methods complement each other, changing the sphere at different sites: • radial keratotomy incisions are applied outside the optical zone, • excimer laser cuts off a peace of cornea in the optical zone. • Methods become technically simpler: • imperfect correction by RK may be later compensated by laser • laser manipulations on thin corneas become safe
2006 – 2008 The idea applied
Equipment used • Surgery • Allegretto Wave Eye-Q • Zyoptix XP microkeratome • Leica M841 microsurgical microscope • Microkeratomes for radial keratotomy both American and Russian styles • Diagnostics • ALLEGRO Topolyzer • ALLEGRO Analyzer • Pachymeters • Humphrey ultrasonic pachymeter • Qvantel Medical POCKET II pachymeter • Heidelbeg Engineering pachymeter
Our method for combined correction • Patients • total: 31 patients • with thin corneas (about 500 m) • Initial myopia: -7D to -14D • too high to correct by single step RK • Two steps: • first - ”soft” RK • followed by excimer laser (LASIC or PRK-like) correction when the cornea is completely stabilized • interval between steps: 11 - 18 months • Results: eumetropia in all cases. • Not a single case of keratoconus was noted, even in risk patients.
Contact lenses in between • Since fast patient rehabilitation is paramount in vision correction, we recommended our patients to wear contact lenses early, in 4-5 weeks after the first step. • 24 patients agreed to constant wear of silicon-hydrogel contact lenses, • at the beginning Bausch & Lamb Pure Vision lenses (base curve 8,6) were used, • later we switched to CIBA VISION Air Optix Night & Day (base curve 8,4;8,6). • These lenses were very well tolerated after surgery, had the advantage of constant wear.
Observation 3 • In addition in the 24 patients we observed permanent decrease of astigmatism (due to post-operative corneal plasticity?). • Average improvement was 0,75D. • The lower degree of astigmatism allowed to enlarge the excimer correction zone and thus ensure better nigh vision.
Controls • We have a group of 81 patients available for comparison, who: • did not achieve eumetropia after RK • and wore soft-hydrogel lenses. • In addition, there is a group of 7 patients who refused lenses between the first and second steps of combined correction. • We haven’t found detectable permanent changes of astigmatism status in both groups.
(preliminary!!) Conclusions
Probable mechanisms • Cornea after RK is not rigid and remains bendable by weak but constant pressure for about half a year. • Application of dense silicon-hydrogel contact lenses at the time of increased corneal plasticity produced an effect that is similar to orthokeratology, but permanent.
The role of lenses • Difference between Bausch & Lamb and CIBA VISION for our patients is being evaluated. • Further molding of the cornea could be achieved by orthokeratology methods • that, in contrast to a normal eye, should produce permanent effect in this case.
Benefits • The use of dense contact lenses at the intermediate stage between the surgeries seems to be very promising. • Gentle unpretentious RK that doesn’t aim at perfect and complete correction could be used as the first step for shaping the corneal surface. • In that way, RK will be easily manageable by most ophthalmic surgeons. • Additional indications for excimer laser surgery could appear and better results for patients with difficult eye anatomy should be expected.