Download
1 / 24
250 likes | 520 Views
Cervical Screening and HPV testing. Dr Tracy Owen Quality Assurance Director, NICSP. Aim of screening. To reduce mortality and morbidity associated with cervical cancer by identifying and treating pre-cancerous changes Screening can prevent 70% of cervical cancers

E N D
Cervical Screening and HPV testing • Dr Tracy Owen • Quality Assurance Director, NICSP
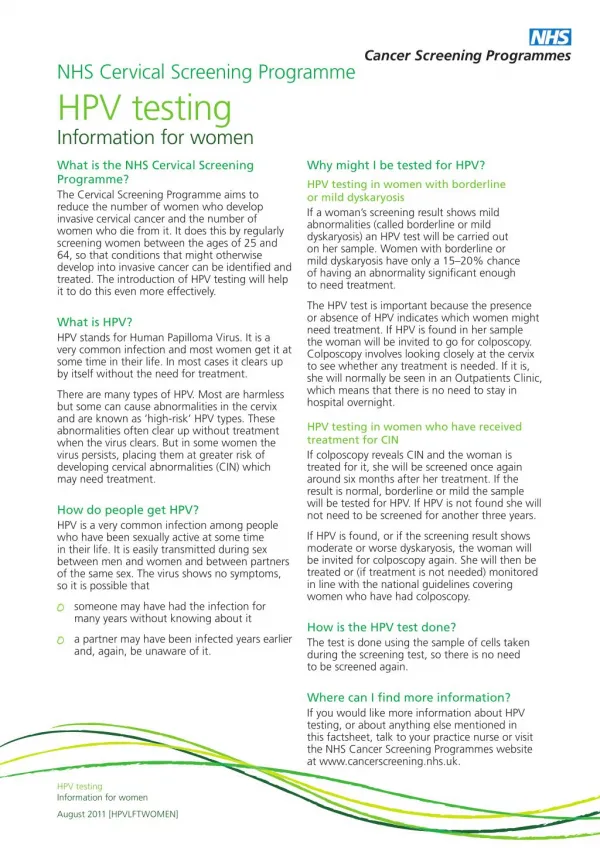
Aim of screening • To reduce mortality and morbidity associated with cervical cancer • by identifying and treating pre-cancerous changes • Screening can prevent 70% of cervical cancers • Liquid based cytology – introduced 2007/08 • ? Role of HPV testing in screening pathway - HPV detected in 99.7% of cervical cancers
Coverage rates by Trust NI coverage = 77.32% (2010/11) Coverage = % of eligible women with a screening result in last 5 years
Is there anything else that you can do to improve informed choicein your practice?
Reminder - policy change • From Jan 2011 Evidence based, endorsed by UK National Screening Committee, in line with WHO recommendations
What do we know about HPV? • >100 types – only small number cause cervical cancer (HR-HPV) • Transient infection very common - 8 in 10 people infected in lifetime • Prevalence decreases with age (Manchester study) • 40% of 20-24yr olds with HR HPV, 5% of 60-64 yr olds • Can’t be treated but can clear on its own • Infection persists in 20-30% of women
HPV – a complicated issue • Women or their partners may have HPV for many years without knowing it • 99% of cervical cancers associated with persistent infection with high risk types of HPV (70% linked to HPV 16 or 18). • Transmitted by close skin-to-skin contact • Condoms help but don’t provide full protection
HPV testing and screening • HR-HPV testing at two points in screening pathway - Triage and Test of Cure • Improved management of ‘low grade’ abnormalities • Introduced for smears taken from Monday 28 January 2013 • Applies to women in screening age range (25-64 yrs) • HPV test is carried out on the same sample
HPV triage • 15-20% of women with borderline/mild changes have a significant abnormality that needs treatment • HR-HPV testing is effective in identifying which women may need treatment • All borderline/mild samples are tested for HR-HPV (Triage) • HR-HPV positive are referred immediately to colposcopy • HR-HPV negative can be safely returned to routine recall
Benefits of triage • Reduces the need for multiple repeat tests – reduces anxiety & cost • Colposcopy is focused on the women who are more likely to have significant disease • Women get to colposcopy sooner • Negative predictive value of HR-HPV test is reported between 93.8 and 99.7% • ?reduced DNA rate at colposcopy
STANDARD PROTOCOL HPV TRIAGE PROTOCOL
Test of Cure (TOC) • To assess women who have been treated for any grade of CIN for risk of having residual or recurrent disease • Women with normal cytology and negative for HR-HPV at follow up are at very low risk of residual disease • HR-HPV test on women with normal, mild or borderline cytology result at 6 month follow up after treatment (excluded if treated for CGIN/invasive disease) • If HR-HPV negative are returned to routine recall • If HR-HPV positive are referred back to colposcopy
Benefits of TOC • Approx 80% of treated women avoid annual cytology tests • Cost savings to primary care and laboratory • Improved service for women - shorter patient journey time with return to routine recall
STANDARD PROTOCOL HPV TOC PROTOCOL
Information forsmear takers • Packs issued to all practices • **ensure all smear takers in practice have seen this**
HPV testing will be done as appropriate on same sample – you do not need to request it • Cytology and HPV result will be issued on same report • Patient consent • Be prepared to answer patient questions • risk of cancer • transmission of HPV
Psychological impact of HPV infection • Surprise and anxiety. • Guilt and shame are closely linked to concerns about transmission and disclosure to future sexual partners. • Providing clear and accurate information to women can considerably reduce the anxiety they experience and the possible stigma associated with HPV. • Women should be assured that having sex just once exposes them to many subtypes of HPV and this exposure should be viewed as normal.
Terminology • Women are frequently confused by the term ‘wart virus’. It is incorrect and should be avoided. • Using the term ‘HPV positive’ can arouse concern and may be confused with ‘HIV positive’. • Result letters should indicate that ‘high-risk HPV’ has been detected.
How do I protect myself against HPV? • HPV infection cannot be treated, only CIN. • Attend cervical screening regularly. • Vaccination is now available to protect against 16, 18 subtypes. • HPV vaccination will help to prevent HPV infection/CIN in the future.
Further information/contact • Quality Assurance Reference Centre (QARC) • Public Health Agency • 18 Ormeau Avenue • Belfast • Tel: 028 9027 9381 • www.cancerscreening.hscni.net • www.cancerscreening.nhs.uk