Download
1 / 27
280 likes | 376 Views
Essential Thrombocythemia Followed by Acute Leukemia. Does therapy lead to leukemic transition or is it a failure of accurate diagnosis?. Joel Saltzman MD Hematology/Oncology Fellow Metro Health Medical Center. 63 yo male admitted with Appendicitis.

E N D
Essential Thrombocythemia Followed by Acute Leukemia Does therapy lead to leukemic transition or is it a failure of accurate diagnosis? Joel Saltzman MD Hematology/Oncology Fellow Metro Health Medical Center
63 yo male admitted with Appendicitis • Diagnosed with Essential Thrombocythemia 1992. Treated with Chlorambucil to keep platelet count less than <600,000K • 1999 diagnosed with AML; cytogenetics normal • Offered induction therapy with 7+3. Pt refused. Continued on Chlorambucil. • Stable AML x 2 years
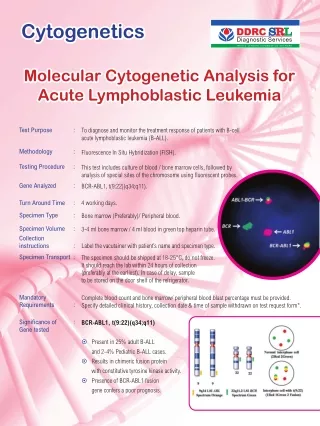
WS labs. • WBC: 14.0, 45% Segs, 7% Bands, 15%Blasts • Plts: 693K • PCR for BCR/ABL +
Objectives • Establish the diagnostic criteria for Essential Thrombocythemia (ET) • Discuss the natural history of ET • Discuss the evidence supporting the treatment of ET • Discuss acute Leukemia following ET
Diagnostic Criteria for ET • Platelet count >600,000 • Hematocrit,40 or normal RBC mass • Normal serum ferritin and MCV • No Philadelphia Chromosome or bcr/abl gene rearrangement • Absence of collagen Fibrosis on bone marrow • No cytogenetic or morphologic evidence for a myelodysplastic syndrome • No cause for reactive thrombocytosis
Presenting Features • Vasomotor symptoms: Erythromelagia • Headache, dizziness, visual disturbances • Thrombosis or bleeding • More common in women • Splenomegaly • Asymptomatic
Pathophysiology • Clonal disorder of a multipotent stem cell which gives rise to erythrocytic, granulocytic, and megakaryocytic series • Cytogenetic abnormalities demonstrated in <25% of patients • Trisomy 8 most common abnormality
Clinical Course • No change in life expectancy • Majority of patients have course complicated by thrombosis and hemorrhage. • Arterial thrombus > venous thrombus • Arterial thrombi more common with smoking, hypertension, coronary artery disease, diabetes mellitus
What is the evidence supporting treatment for ET? Cortelazzo et. al. New England Journal of Medicine, April 1995 • Randomized trial comparing treatment with Hydroxurea to no myelosuppression in 114 Pts with ET at high risk for thrombosis. • Platelet count kept below 600,000 in the treatment group
What defined the High Risk Patient? • Age > 60 years (55%) • Previous history of thrombosis (15%) • Both (30%) • Platelet Count >1,500,000(excluded from randomization because of high risk of bleeding/thrombosis)
Methods • 56 pts randomly assigned to hydroxyurea group. Seen every two weeks until plt count <600,000. Starting dose of hydroxyurea 15mg/kg/day. • 58 patients were the control patients and were seen every two months
Hydroxyurea therapy • Hydroxyurea reduces the incidence of major ischemic episodes from 24% to 3.6% in this high risk patient population
So Why Worry? • Berk et. al. New England Journal of Medicine, 1981, “Increased Incidence of Acute Leukemia in Polycythemia Vera associated with Chlorambucil therapy” • 431 patients randomized to phlebotomy alone, clorambucil, and radioactive phosphorus
Experience of the PVSG with ET • Study the Clonal Myeloproliferative Diseases for the past 20 years • Polycythemia Vera • Essential Thrombocythemia • Chronic Myeloid Leukemia • Myelofibrosis
Modifications in the Diagnostic Criteria for ET • Used to include stainable iron in marrow • Now a normal or increased ferritin is accepted to r/o Iron Deficiency • Absence of bcr/abl gene rearrangement or Philadelphia chromosome • No cytogenetic or morphologic evidence of MDS. Absence of 5q- or ringed sideroblasts
Presenting Characteristics of 100 patients with original criteria • PVSG chose only patients with plts> million. (9 were excluded) • 50/91 met all the newly established criteria for ET • 41 patients patients did not meet all established criteria. • Three major problems were found in these 41 patients
Major difficulties with 41pts • Iron deficiency not rule out (28 pts) • Polycythemia Vera was not formally excluded (9pts) • Lack of karyotypic analysis to exclude Philadelphia chromosome
Lack of bone marrow karyotype adequate to rule-out PH1 • 18 patients lacked this analysis • 6 of these patients eventually had karyotypic analysis consistent with CML. Most progressed to chronic phase CML and 5/6 progressed to acute blastic leukemia • It is now recognized that some CML patients will have bcr/abl without chromosomal abnormality
Patients were placed in 4 prospective trials • Protocol 54:randomization between radioactive phosphorus and Melphalan • Protocol 10: same as above except increased dose of 32P • Protocol 12: Hydroxyurea • Seven patients were simply followed without treatment
PVSG experience with Hydroxyurea in ET • 29/91 of these initial patients were enrolled in PSVG-12 • 6/29 developed acute leukemia • No major differences were observed between the two groups were noted
Conclusions • Hydroxyurea remains the treatment of choice for patients at high risk for the thrombotic complications or at risk for them • Low incidence of acute leukemias in patients treated with HU alone, suggests the lack of a leukemogenic effect • Accurate diagnosis of ET is essential to long term management (I.E. send RT PCR for BCR/ABL)