Download
1 / 88
910 likes | 1.55k Views
PHARYNX & OESOPHAGUS 1. By Prof. MOHAMED A. EL GHARBAWI Web site: www.dr-elgharbawi.com e-mail: elgharma2@yahoo.com. ILOs. By end of this lecture, you should know Causes of dysphagia Hypopharyngeal (Post-cricoid) carcinoma Pharyngeal diverticulum (Pouch) Surgical anatomy of oesophagus

E N D
PHARYNX & OESOPHAGUS 1 By Prof. MOHAMED A. EL GHARBAWIWeb site: www.dr-elgharbawi.com e-mail: elgharma2@yahoo.com
ILOs By end of this lecture, you should know • Causes of dysphagia • Hypopharyngeal (Post-cricoid) carcinoma • Pharyngeal diverticulum (Pouch) • Surgical anatomy of oesophagus • Achalasia of oesophagus • Diffuse oesophageal spasm • Gastro-esophageal reflux disease • Hiatus hernia
DYSPHAGIA • DEFINITION:Pain or difficulty during the act of swallowing • ETIOLOGY:A. Causes in Mouth: 1. Congenital: Cleft palate 2. Traumatic: Wounds & Fractures 3. Inflammatory: Stomatitis, Glossitis & Ulcers 4. Neoplastic: Carcinoma
DYSPHAGIA • ETIOLOGY (Cont.):B. Causes in Pharynx: 1. Congenital: Stenosis of pharynx 2. Traumatic: Foreign Body (FB), Corrosives 3. Inflammatory: Pharyngitis, Tonsillitis, Diphtheria , Quinzy & Retropharyngeal abscess 4. Neoplastic: Post-cricoid carcinoma 5. Functional: Pharyngeal pouch Neuromuscular disturbance e.g. Myopathy
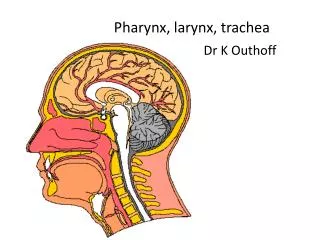
DIVISIONS OF PHARYNX Nasopharynx, Oropharynx & Laryngopharynx
DYSPHAGIA • ETIOLOGY (Cont.):C. Causes in esophagus: 1. Congenital: Atresia, Short esophagus, Dysphagea lusoria 2. Traumatic: FB, Corrosive (Benign stricture) 3. Inflammatory: Plummer Vinson’s Syndrome Reflux esophagitis & Hiatus hernia 4. Neoplastic: Benign & Malignant tumors 5. Functional: Achalasia of cardia
DYSPHAGIA • ETIOLOGY (Cont.):D. Causes outside esophagus (External pressure): I. In neck: 1. Goiter (Thyroid swelling) 2. Lymphadenopathy 3. Tumors 4. Adhesions II. In Thorax: 1. Double aortic arch ( Dysphagia losuria) 2. Mediastinal syndrome
DYSPHAGIA • ETIOLOGY (Cont.):E. General Causes: 1. Tetanus 2. Rabies 3. Bulbar paralysis 4. Myasthenia gravis 5. Hysterical dysphagia
POST CRICOID CARCINOMA(Hypopharyngeal Carcinoma) • Incidence:One of the common tumors in EgyptCommon in females • Predisposing factor:Plummer Vinson’s Syndrome • Pathology:This is a tumor of LaryngopharynxSite: Arises from the mucous membrane lining the pharynx at the level Cricoid cartilage (Anteriorly, laterally or posteriorly)
POST CRICOID CARCINOMA(Hypopharyngeal Carcinoma) • Pathology ( Cont.):Macroscopy: 3 types 1. Ulcer type 2. Cauliflower type 3. Stricture typeMicroscopy:Squamous cell carcinoma • Clinical Picture:* Common in middle aged females (40’s)* Complaint: Progressive dysphagia, first to solids then to fluids Patient can finger point the level of obstruction
POST CRICOID CARCINOMA(Hypopharyngeal Carcinoma) • Clinical Picture (Cont.):* Hoarseness of voice & Dyspnea occur later with involvement of larynx* Localpain or referred to ear* In advanced cases, larynx is pushed forward & a mass may be feltbehind it* Loss of the normal click felt on moving larynx sideway
POST CRICOID CARCINOMA(Hypopharyngeal Carcinoma) • Investigations: 1. Pharyngoscpoy shows the tumor & takebiopsy 2. Barium swallow3. CT with or without contrast • Treatment:Operable cases: Total laryngo-pharynectomy (Larynx & Pharynx with block neck dissection en mass)Resulting in Tracheostomy & esophagectomyReconstruction may be done laterInoperable cases:Palliative gastrostomy & Tracheostomy+ Irradiation
PHARYNGEAL POUCH (ZENKER’SDIVERTICULUM) • Etiology:*It is a pulsion diverticulum at the posterior pharyngeal wall*Two factors are sharing in etiology1. Presence of a weak area in the posterior pharyngeal wall known as Killian’s dehiscence (It is located between the upper oblique part & the lower transverse part of the inferior constrictor muscle of the pharynx)2. Intrapharyngeal pressure due to achalasia (failure of relaxation) of cricopharyngeus ms. duringswallowing
KILLIAN’S DEHISCENCE(Weak area in the posterior pharyngeal wall)
PHARYNGEAL POUCH (DIVERTICULUM) • Pathology:* It begins posteriorly in midline.* When it becomes bigger, it deviates to one side (usually left side).* Composed of mucous membrane from inside & fibrous tissue outside.* Due to the associated spasm of cricopharyngeus ms, food passes easier to it than to esophagus • Clinical picture: History:*Elderly males* Progressive dysphagia & regurgitation of undigested food* Weight loss & malnutrition (Advanced cases)
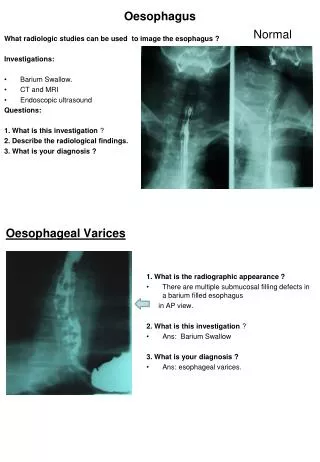
PHARYNGEAL POUCH (DIVERTICULUM) • Clinical picture: Local Examination:*May be a swelling present in the posterior triangle of the neck*Usually on the left side*It soft & compressible*Enlarges with eating or drinking • Investigations:*Barium swallow: A flask-shaped pouch with fluid level *Esophagoscopy: It shows the opening of the pouch
PHARYNGEAL POUCH (DIVERTICULUM) • Treatment: 1. Endoscopic Stapling ( Minimally Invasive Surgery) It is a recent minimally invasive procedure. Endoscopic linear stapler is used to anastomose thefront of the diverticulum to the back of the esophagus. The staple cuts the crico-pharyngeus muscle at the same time, treating the cause.2. Surgical excision of the diverticulum + Myotomy of the cricipharyngeus muscle.
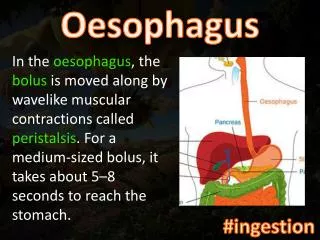
OESOPHAGUS(ANATOMY ) • Surgical Anatomy: *25 cm long fibromuscular tube * Extending from C6 to T10 vertebrae* Located in posterior mediastinum*Upper 1/3rds with striated muscle fibers &Lower 2/3rds with smooth muscle fibers* Lined by stratified squamous epithelium* Its abdominal part is lined with gastric mucosawithout oxyntic or peptic cells
OESOPHAGUS(ANATOMY ) • Blood supply: * Cervical part: From inferior thyroid arteries* Thoracic part : From Aorta & Bronchial arteries* Abdominal part: From Lt gastric artery • Venous drainage: * Drainage to Inferior thyroid veins, Azygos & Leftgastric vein.* Venous plexus around the lower esophagus is one site of portsystemic communications • Lymphatic drainage:* Cervical part: Drains to the cervical L Ns* Thoracic part: Drains to the mediastinal & tracheo- bronchial LNs* Lower part: Drains to Lt gastric & celiac LNs
OESOPHAGUS(PHYSIOLOGY ) • No absorption • No enzymatic secretion or digestive activity • Only functionis food transmission through the tube • Body of esophagus reflects the normal negative intrathoracic pressure • Negative intraluminal esophageal pressure • Sphincters at both ends of esophagus have resting tone. • This sphincters tone prevents air, solids or fluids frompassing in or out under resting conditions.
OESOPHAGUS(PHYSIOLOGY ) • Sphincters:A. Cricopharyngeal sphincter zone: 2-3 cm. long, resting pressure is 30 cm. waterB. Gastro-esophageal zone: 3-4 cm. long, resting pressure is 15-25 cm. waterC. Competence of Gastro-esophageal junction depends on the following factors: 1. Acute angle of Hiss: The valvular effect of the acute esophago-gastric angle 2. Pinchcock action of the right crus of diaphragm 3. “Rosette like” folds of the gastric mucosa at cardia 4. About 3-4 cm. of esophagus are intra-abdominal with positive pressure 5.Circular muscle fibers at lower end of esophagus 6. A band of smooth muscle in the fundus of stomach, working as a sling, to accentuate the esophago-gastric angle
OESOPHAGUS(NEUROMUSCULAR DISORDERS ) ACHALASIA OF CARDIA (Cadriospasm) • Etiology:1. Cause is unknown2. May be due to degeneration of Auerbach’s plexus3. Chagas’s disease ( Infection with Trypanosoma Cruzi) in South America, may cause a similar degeneration & produce motor changes similar to those of Achalasia • Pathophysiology: Motility disorder in Achalasia includes 1. Absencent propulsive peristalsis allover the esophagus2. Failure of the lower esophageal sphincter to relax on swallowing
OESOPHAGUS(NEUROMUSCULAR DISORDERS ) ACHALASIA OF CARDIA (Cadriospasm) • Incidence:A common motility disorderFemales = MalesMost common in middle ageMay occur in any age
OESOPHAGUS(NEUROMUSCULAR DISORDERS ) ACHALASIA OF CARDIA (Cadriospasm) • Clinical picture:1. Some patients may have psychoneurotic disorder2. Dysphagia is the main symptom: CharacteristicsIntermittentcourse To Fluids > Solids (weight of solids can force the sphincter to open)Long duration may lead to weight loss3. Sense offullnessbehind the lower end of sternum4. Regurgitation during sleep may lead to aspiration pneumonia
OESOPHAGUS(NEUROMUSCULAR DISORDERS ) ACHALASIA OF CARDIA (Cadriospasm) • Investigations:1. CXR & Upper abdomen: *Fluid level behind the heart * Absence of air bubble in the stomach2. Barium swallow & Meal: * Normal in early cases * In advanced cases: Dilated esophagus (Sigmoid like esophagus) Full of barium & food debris Tapering smoothly to the cardia (Hen’s beak or Bird’s beak appearance)
ACHALASIA OF CARDIABarium swallow (Tapering smoothly to cardia)
OESOPHAGUS(NEUROMUSCULAR DISORDERS ) ACHALASIA OF CARDIA (Cadriospasm) • Investigations (Cont.):3. Esophagoscopy: The endoscpoe can be advanced easily through the narrow sphincter without increased force. Thisdifferentiates Achalasia from Carcinoma or benign peptic ulceration4. Endoscopic US shows thickening of muscle in the esophageal wall5. Esophageal Manometry: 2 abnormalities are essential: * Failure of the lower esophageal sphincter to relax in response to water bolus swallow * Weak peristalsis of esophageal wall
OESOPHAGUS(NEUROMUSCULAR DISORDERS ) ACHALASIA OF CARDIA (Cadriospasm) • Treatment:1. Medical Treatment: May be beneficial in early cases. * Psychotherapy * Antispasmodics2. Dilatation: Symptoms are relieved in 80% of cases. * Use: Mercury loaded bougie Or Hydrostatic bag. * The hydrostatic bag is distended with water when it lies in the cardiac end. Aiming at rupture of the muscle coat in the spastic area. * This may be complicated with perforation of esophagus3. Surgery: * Heller’s operation ( Cardiomyotomy) is the best. * Divide the muscle coat longitudinally until mucosa bulges. * Similar to pyloromyotomy. * Approach: Through the abdomen or thorax. * Results: Good, Esophageal reflux is absent or minimal. * Anti reflux procedures may be added.4. Laparoscopic or Thoracoscopic (Minimal invasive): To do same operation.
ACHALASIA OF CARDIALaparoscopic Cardiomyotomy .Heller’s operation
OESOPHAGUS(NEUROMUSCULAR DISORDERS ) Diffuse Esophageal Spasm (CORKSCREW ESOPHAGUS) • Definition:Frequent simultaneous, repetitive & prolonged spasm of the esophagus in response to swallowing. It does not occur in resting condition. • Unknown etiology. • It is uncommon condition • It causes chest pain rather than dysphagia • Its pain resembles that of myocardial ischemia • Investigations: * Barium swallow & meal may show segmental contraction of esophagus. In sever spasm, it may show Corkscrew appearance In many cases, it may be reported as normal * Endoscopy is usually normal • Treatment: * Antispasmodics to reduce smooth muscle tone may have success * Long esophageal myotomy from aortic arch to the cardia
DIFFUSE OESOPHAGEAL SPASMBARIUM STUDY ( CORKSCREW OESOPHAGUS)
OESOPHAGUS(GASTRO-ESOPHAGEAL REFLUX DISEASE )GERD/GORD • Incidence:1. It occurs normally after meals (Physiology)2. It is considered as a disease if the attacks become more frequent & prolonged causing effects on esophageal mucosa3. It is the commonest upper GI disorder4. It affects 45% of population with variable degrees • Pathophysiology:Mechanisms that prevent reflux & its harmful effects are * Factors maintaining competence of Gastro-esophageal junction are discussed before * Esophageal clearance of the refluxing gastric fluids area. Normal peristalsis of the esophagus during swallowing b. The swallowed saliva is alkaline that neutralizes the acidic refluxing gastric fluid
OESOPHAGUS(GASTRO-ESOPHAGEAL REFLUX DISEASE )GERD/GORD • Etiology:GERD may occur due to: 1. Incompetence of gastro-esophageal junction as a result of failure of the above mentioned protective mechanisms2. Gastric distention or Delayed gastric emptying (Some food cause delayed gastric emptying e.g. fatty meal Coffee & Chocolate) Also may be due to gastric outlet obstruction
OESOPHAGUS(GASTRO-ESOPHAGEAL REFLUX DISEASE )GERD/GORD • Complications:GERD may occur due to: 1. Esophagitis with erosion & ulceration2. Stricture of esophagus 3. Barrett’s esophagus It is columnar metaplasia (normally Stratified squamous epithelium) of the lower esophageal mucosa as a result of chronic irritation. It is a premalignant condition.
OESOPHAGUS(GASTRO-ESOPHAGEAL REFLUX DISEASE )GERD/GORD • Clinical picture: 1. Typical picture: Triad of heart burn + regurgitation+ Dysphagia It is increasing after meals, by night & when the patient lies flat or lean forward.2. Atypical presentation: * Chest pain (may be mistaken for Angina) * Chocking episodes & cough * Bronchial asthma * Hematemesis (rare)