Download
1 / 31
320 likes | 761 Views
Evaluating Testicular Pain. Kaveh Mansuripur Ambulatory Medicine Clerkship 4/9/09. Learning Objectives. By the end of the session, be able to: List the differential dx for testicular pain Label or draw the relevant anatomy

E N D
Evaluating Testicular Pain Kaveh Mansuripur Ambulatory Medicine Clerkship 4/9/09
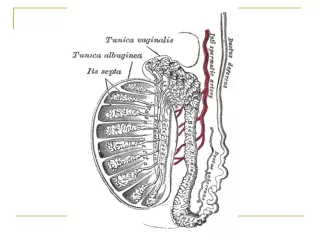
Learning Objectives By the end of the session, be able to: • List the differential dx for testicular pain • Label or draw the relevant anatomy • Describe the physical examination appropriate for a patient with testicular pain • Select appropriate testing for patients with testicular pain in context of specific sxs and signs • Select the most appropriate treatment for patients with specific causes of testicular pain
Case 1: Patient T.R.What is the Differential Diagnosis? HPI: 21 yo man presents with 3 hours of intense, constant testicular pain Began several hours after college track meet Associated nausea and vomiting PMH: None Meds: Glucosamine, condroitin, creatine supplements Alls: PCN FH: Non-contributory SH: Sexually active, multiple partners
Differential Diagnosis • Testicular Torsion • Appendiceal Torsion • Epididymitis • Trauma • Inguinal Hernia • Henoch-SchonleinPurpura • Mumps • Fournier’s Gangrene • Referred Pain
Case 1: Patient T.R. • Exam:
Case 1: Patient T.R.What is the Next Step? Exam: • Right testicle higher than left • Long axis oriented horizontally • Significant swelling • No cremasteric reflex on either side • No relief of pain on elevation
Case 1: Patient T.R.Next Step If Diagnosis Certain (Torsion): • To the OR. • Outcomes directly related to length of time from onset • Irreversible ischemia at mean of 12 hours If Diagnosis Less Obvious • Doppler Ultrasound • Test 82% sensitive, 99% specific for torsion (loss of flow)
Case 1: Patient T.R. Operation: • testicular detorsion and fixation • Unilateral or bilateral? Why?
Case 1: Patient T.R. Operation • testicular detorsion and fixation • Unilateral or bilateral? Why? ANSWER: Bilateral-- Torsion associated with absence/insufficeincy of gubernaculum. Often bilateral. What if surgery not an option?
Case 1: Patient T.R. Non-operative: Manual detorsion • 2/3 of cases are torsed medially, 1/3 laterally • Success marked by decreased pain, return to normal position. • If unsuccessful, apply ice (successful in animal models)
Testicular Torsion • 40% over 21 • Associated with physical activity/sleep • Exam • Absent cremasteric • Doppler • Surgical Emergency
Case 2: Patient F.J. HPI: • 11 year old boy presents with 3 days of increasing scrotal pain • Localizes tenderness to anterior superior pole of right testicle • dDx?
Case 2: Patient F.J. Exam
Case 2: Patient F.J. Exam: • Tender as reported • Transillumination: hydrocele at AS pole • Cremasteric reflexes intact bilaterally • Discoloration visible externally as sub-centimeter dot at site
Case 2: Patient F.J. Further tests?
Case 2: Patient F.J. Further tests? • Ultrasound will show focus of decreased echogenicity at site Treatment?
Case 2: Patient F.J. Further tests? • Ultrasound will show focus of decreased echogenicity at site Treatment? • Conservative • Ice, anti-inflammatory medications • Pain resolves in weeks-months • Residual nodule • Operative • Low risk • Recovery in days
Appendiceal Torsion • 80% between 7-14 years • Leading pediatric scrotal pathology • Gradual onset • Tenderness localized to AS aspect • Intact cremasteric reflex • “Blue Dot” sign in 21%
Case 3: Patient J.D. CC: 31 yo man with Testicular Pain HPI • 5 days, waxing/waning. Began several hours after exercise. No previous episodes. • Left testicle, some radiation to L. inguinal fold, L. gluteal region • “Achy” in quality; 4-8/10 • No N/V/F/C or other associated symptoms • ED visit 3 days ago. Clean U/A at time. Told to FU outpatient if pain unresolved.
Case 3: Patient J.D. PMH Noncontributory Meds None Allergies NKDA FH/SH HTN, MI in father 1ppd, social EtOH, bisexual.
Case 3: Patient J.D. Exam • Mild swelling around left testicle • Normal lie • Tenderness localizes to PS pole WHAT IS DIFFERENTIAL DIAGNOSIS?
Case 3: Patient J.D. Exam • Mild swelling around left testicle • Normal lie • Tenderness localizes to PS pole Diagnosis: • Epididymitis
Case 3: Patient J.D. Bacterial Epididymitis • What to give and why?
Case 3: Patient J.D. Bacterial Epididymitis • What to give and why? • C. trachomatis and N. Gonorrhea most common in men under 35
Case 3: Patient J.D. Bacterial Epididymitis • What to give and why? • C. Trachomatis and N. Gonorrhea most common in men under 35 • Doxycycline 100mg PO BID x10 days • Ceftriaxone 250mg IM x1
Case 3: Patient J.D. Bacterial Epididymitis • What to give and why? • C. Trachomatis and N. Gonorrhea most common in men under 35 • Doxycycline 100mg PO BID x10 days • Ceftriaxone 250mg IM x1 • Coliforms?
Case 3: Patient J.D. Bacterial Epididymitis • What to give and why? • C. Trachomatis and N. Gonorrhea most common in men under 35 • Doxycycline 100mg PO BID x10 days • Ceftriaxone 250mg IM x1 • Coliforms? • Quinolones (ofloxacin 300mg PO BID x10 days)
Epididymitis • Mostly subacute • ABX • Evaluate recurrent cases for GU malformation • Acute more common in older men, prostatitis • Fever, chills, GU symptoms
References • Edelsberg, JS, Surh, YS. The acute scrotum. Emerg Med Clin North Am 1988; 6:521. • Eyre, RC. Evaluation of the acute scrotum in adult men. In: UpToDate, Basow, DS (Ed), UpToDate, Waltham, MA, 2008. • Fisher, R, Walker, J. The acute paediatric scrotum. Br J Hosp Med 1994; 51:290.