Download
1 / 52
580 likes | 1.24k Views
Ventricular Septal Defects. Echo Conference 5/11/11 Darryn Appleton. Outline. Morphology, Types & Pathophysiology Natural History and Clinical Presentation Some Echo examples Clinical Scenarios and Recommendations Interventions: Indications, Surgery, Percutaneous

E N D
Ventricular Septal Defects Echo Conference 5/11/11 Darryn Appleton
Outline • Morphology, Types & Pathophysiology • Natural History and Clinical Presentation • Some Echo examples • Clinical Scenarios and Recommendations • Interventions: Indications, Surgery, Percutaneous • Pregnancy and Endocarditis Prophylaxis • Review Questions
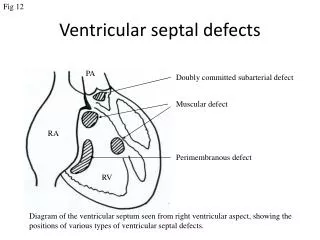
Introduction • The most common form of CHD, accounting for up to 20-40% of patients diagnosed with CHD • Impact may range from asymptomatic to pulmonary HTN, LV volume overload and RVH • Morphology: 4 types • Membranous – most common type in adults (80%) • Muscular – most common type in young children • Complete AV septal (endocardial cushion) defects • Supracristal (subarterial)
Morphology – The Ventricular Septum • Membranous • Outflow • Trabecular septum • Inflow • Subarterial / Supracristal
Pathophysiology • Defect size is often compared to aortic annulus • Large: > 50% of annulus size • Medium: 25-50% of annulus size • Small: <25% of annulus size
Pathophysiology • Restrictive VSD is typically small, such that a significant pressure gradient exists between the LV and RV (high velocity), with small shunt (Qp/Qs ≤ 1.4 : 1) • Moderately restrictive VSD moderate shunt (Qp/Qs 1.4 to 2.2 : 1) • Large / non-restrictive VSD large shunt (Qp/Qs > 2.2 : 1) • Eisenmenger VSD irreversible pulmonary HTN and shunt may be zero or reversed (i.e. RL)
Natural History • Restrictive: typically does not have hemodynamic impact and may close spontaneously • Location Location Location: Subaortic may result in progressive AI • Moderately restrictive: does create LV overload and dysfunction along with variable increase in PVR • Large / non-restrictive: LV volume overload earlier in life with progressive pulm HTN and ultimately Eisenmenger syndrome
Clinical Features • Peds: • Murmur • Dyspnea, CHF, Failure to thrive • Adults: • Asymptomatic murmur – harsh, pansystolic, left sternal border • Mod restrictive – dyspnea, a.fib, displaced apex, murmur, S3 • Non-restrictive Eisenmenger VSD – central cyanosis, clubbing, RV heave, loud P2
t Outlet VSD – Para long axis
Echo Example 3 Membranous • Type: • Size: Restrictive
Echo Example 3 Type: Size: Shunt: Muscular Large / Non-restrictive • RL (inc RH pressures) • RV dilated • Eisenmengers
Clinical Scenarios & Recommendations • Symptomatic young infant with Pulm HTN • Early surgery within 3 months. • Medical therapy with diuretics +/- ACEI pre-op • Asymptomatic pt without Pulm HTN but with LV overload • Closure usually recommended to avoid late LV dysfunction • Asymptomatic pt, small VSD, no LV dilation • Conservative • Asymptomatic pt, small VSD but with AI/prolapse • Peri-membranous VSD with more than trivial AI should have surgery
Clinical Scenarios & Recommendations • Eisenmenger Syndrome • Supportive • Bosentan (Endothelin receptor antagonist) – improves functional capacity, QOL • Sildenafil Penny DJ, Vick GW. Lancet 2011; 377: 1103-12
Interventions • Indications for Surgical Closure in adults: • Evidence of LV volume overload (Class I if Qp/Qs >2, Class IIa if Qp/Qs > 1.5) • History of bacterial endocarditis (Class I) • Significant LR shunt with PA pressure < 2/3 systemic and PVR is < 2/3 SVR • Surgical Closure • Considered the first-line choice of therapy for those with indications • Usually involves direct patch closure w cardio-pulm bypass • Operative mortality < 2% in most centers
Long Term Surgical Outcomes • Retrospective review of 46 pts with surgical VSD repair at Mayo Clinic Mongeon et al. JACC Int 2010; 3: 290-7
Interventional Options • Percutaneous Device Closure • Muscular VSDs can typically be closed percutaneously • Class IIb recommendation in Guidelines (i.e. surgery still preferred) • No FDA approved devices for perimembranous VSDs, although there are specific devices for this purpose • Concern re proximity of defect to AV node and high risk of complete AV block requiring pacemaker
Pregnancy and VSDs • Pregnancy well tolerated in women with small to moderate sized VSDs as long as there is no pulmonary vascular involvement • Eisenmenger syndrome: Pregnancy contraindicated due to exceptionally high risk of maternal and fetal death
Endocarditis Prophylaxis for VSD • Uncomplicated VSD – no Abx for dental or other procedures required • Post repair: • Abx for 6 months following surgical or percutaneous repair • Indefinite Abx if there is residual shunt • Risk of bacteremia from daily life usually exceeds that of procedure Abx for procedures only prevent small % of cases • Focus should be on optimal dental hygiene for those with CHD
Question 1 • An isolated VSD will generally cause enlargement of which chamber(s): • A: Left atrium, left ventricle • B: Right ventricle • C: Right ventricle, pulmonary artery • D: Aorta • E: Right ventricle, right atrium
Question 1 • An isolated VSD will generally cause enlargement of which chamber(s): • A: Left atrium, left ventricle • B: Right ventricle • C: Right ventricle, pulmonary artery • D: Aorta • E: Right ventricle, right atrium
Question 2 • The defect shown on the previous slide is a: • A: Muscular VSD • B: Sinus venosus VSD • C: Perimembranous VSD • D: Inlet VSD • E: Supracristal VSD
Question 2 • The defect shown on the previous slide is a: • A: Muscular VSD • B: Sinus venosus VSD • C: Perimembranous VSD • D: Inlet VSD • E: Supracristal VSD
Question 3 • A common complication of this defect is: • A: Pulmonary valve endocarditis • B: Aortic regurgitation • C: Aortic dissection • D: Tricuspid regurgitation • E: Right ventricular enlargement
Question 3 • A common complication of this defect is: • A: Pulmonary valve endocarditis • B: Aortic regurgitation • C: Aortic dissection • D: Tricuspid regurgitation • E: Right ventricular enlargement
Question 4 • There is no diastolic flow in this perimembranous VSD • A: True • B: False
Question 4 • There is no diastolic flow in this perimembranous VSD • A: True • B: False
Question 5 • A restrictive VSD is a simple lesion with a good long term prognosis. However, complications can occur. All of the following are possible complications of a VSD except: • A: Endocarditis • B: Aortic regurgitation • C: Aortic valve prolapse • D: Eisenmenger Syndrome • E: Right sided volume overload
Question 5 • A restrictive VSD is a simple lesion with a good long term prognosis. However, complications can occur. All of the following are possible complications of a VSD except: • A: Endocarditis • B: Aortic regurgitation • C: Aortic valve prolapse • D: Eisenmenger Syndrome • E: Right sided volume overload
Question 6 • The pulmonary artery systolic pressure in this patient with a VSD is: • A: Normal • B: Moderately elevated • C: Systemic / Supra-systemic
Question 6 • The pulmonary artery systolic pressure in this patient with a VSD is: • A: Normal • B: Moderately elevated • C: Systemic / Supra-systemic
Question 7 • A patient with a VSD undergoes TTE. BP measured at the time of the study is 125/75 (right arm), MAP 92. CW doppler across the VSD gives a peak velocity of 5 m/s. Assuming RA pressure of 5, what is the estimated PASP? • A: 20mmHg • B: 25 mmHg • C: 30 mmHg • D: 72 mmHg • E: 105 mmHg