Download
1 / 75
820 likes | 1.32k Views
Study Design. Design of Studies in STD Research. Objectives: Discuss the following study designs: cross-sectional case-control Cohort Clinical trial Discuss the components of study design:

E N D
Design of Studies in STD Research Objectives: • Discuss the following study designs: • cross-sectional • case-control • Cohort • Clinical trial • Discuss the components of study design: • Study Design, population, time frame, inclusion/exclusion, sample size, study flow diagram , outcome/predictors/confounders/effect modifiers, plan of analysis, efforts to reduce threats to validity, strengths/limitations • Discuss some complicated issues in study design
Study Designs Descriptive Analytic Experimental case control correlational clinical trial case report/ case series cohort community trial cross-sectional
Criteria for Causality • Biological Credibility • Consistency of findings • Dose-response • Magnitude of the association • Time sequence
Cross sectional D __ D E __ E
Case Control E D __ E __ D E __ E
Cohort D __ D E D __ E __ D
Phases of a Clinical Trial • Phase I - safety (pharmacokenetics - to determine maximum tolerated dose) • Phase II - Evidence of a response • Phase III - Safety, efficacy • Phase IV - Safety, Acceptability, Efficacy
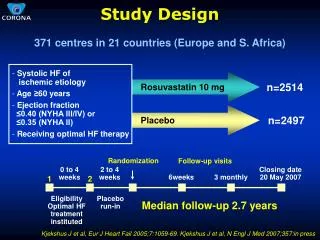
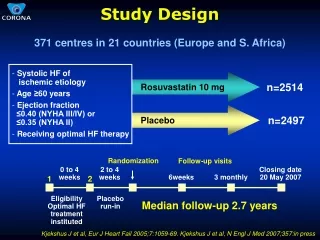
Study Diagram - Classic Randomized Controlled O Eligible Subject Pool Int LTF/C R P/SC O LTF/C
Study Design - Cross-over E E Study Eligibles R C C
Hypothesis Testing • Hypothesis testing involves conducting a test of statistical significance and quantifying the degree to which sampling variability may account for the results observed in a particular study • When designing data collection tools, keep in mind your final analysis Statistical Tests: 2 T-test Measures of Association: Odds Ratio, Relative Risk
Objectives should be stated in terms of an hypothesis • Null Hypothesis: There is no difference Medication A will have not effect on disease progression • Two tailed Hypothesis: There is some difference Medication A will have some effect on disease progression • One tailed Hypothesis: The difference is greater or less Medication A will reduce deaths due to disease X Medication A will increase deaths due to disease X
Outcome of interest • Write the research question in advance • outcome variable: • should be measurable in all subjects • should be capable of unbiases assessments • should be ascertained as completely as possible
Response or Outcome variables • You may have outcomes other than hard endpoints • surrogate markers • quality of life
Follow-up Studies - Survival Analysis • This analysis used when subjects are entered over a period of time and have various lengths of follow-up. • Dichotomous endpoints • Kaplan Meier or Product Limit • Cox Proportional Hazard modeling
Intent-to-treat Analysis • For persons who cross-over to the other arm. You classify that person into the arm they were originally assigned. • Less biased results than “as treated” because you maintain randomization. • Only works if there is not a lot of crossing over very early in the study
Reasons for withdrawal of Subjects • Ineligibility (misclassification, imprisonment, moved) • Noncompliance (adverse effects of intervention, loss of interest, changes in underlying conditions, substance usage)
Measurement • Outcome • Predictor • Confounder • Effect modifier
Validity and Reliability Validity Reliability x xx x
Relative Risk for a disease exposure RR = 75/100 = 3.00 25/100 C.I. (2.10 - 4.29)
Odds Ratio Calculation O.R. = (100*150) = 3.00 (100*50)
Confounding and/or interaction (Kleinbaum, Kupper and Morgenstern)
HIV risk perception and self-protective behaviors among high risk persons in community settings Patricia Kissinger, Ph.D.(1) Nomi Fuchs, MPH (2) Catherine Schieffelin, MPH (2) Jane Herwehe, MPH (2) DeAnn Gruber, MSW (2) (1) Louisiana State University, HIV Outpatient Program (2) Children's Hospital - Family Advocacy, Care and Education Services (FACES)
Purpose • The purpose of this study was to examine HIV risk perception and self-protective behaviors among high risk people in community settings.
Methods • Street intercept and in-depth interviews were conducted from August 1997 to June 1998 • Inclusion: • Sexually active people • aged 15-35 • living in six communities of New Orleans with the highest gonorrhea rates.
Results • Of 1133 respondents, 97% were African American, 37.4% were 15-18 years of age. • 46.2% reported an HIV risk behavior, 66.5% reported condom use, and 69.9% reported ever having been tested for HIV. • Many respondents (39%) perceived themselves to be at no risk, but reported engaging in an HIV risk behavior • Adolescents and persons who had been HIV tested were most likely to have this discrepancy.
Results con’t • Among the 524 persons who reported an HIV risk behavior, 19-35 year olds were less likely to use condoms and adolescent men were less likely to have been HIV tested. • In-depth interviews revealed diverse reasons for failure to perceive oneself at risk and failure to be HIV tested including optimistic bias, risk group identity, hierarchy of risk and fear.
Table 2. Factors associated with a discrepant responsea (N=1072)
Table 3. Factors associated with self protective behaviors among persons reporting an HIV risk behavior (N=524)
Table 4 Association between reported risk behavior and self-assessed risk
Non-experimental (analytic) study designs • Conducted because of ethics, cost or convenience • Two primary types: • Cohort • Case-control
Experimental Designs • Experiment– a set of observations, conducted under controlled circumstances, in which the scientist manipulates the conditions to ascertain what effect such manipulation has on the observations. • Ideally only one factor is examined (however, biological variation exists) • Clinical Trials – (individual in a special environment are randomized) • Field Trials – (individuals in the community are randomized) • Community Interventions – (whole communities are randomized)
Field Trials • Differ from clinical trials in that subjects have not yet gotten disease • (1955) Salk vaccine for Polio • (1975) Vitamin C in preventing the common cold) • (1982) MRFIT – a field trial of several primary preventives of MI (N=12,866 and cost $115 million)
Community Intervention and Cluster Randomized Trials • Community intervention is an extension of a field trial that involves intervention on a community-wide basis • (eg. Mass media campaigns) • (eg. Fluoridated water) • Cluster randomization - groups of participants are randomized. The larger the cluster, the less that is accomplished by randomizing.
Study Protocol • Rationale and background • Objectives • Study Design • Inclusion/Exclusion • Definitions (intervention, measurements, adherence) • Study Flow chart • Sample Size calculation • Plan of analysis (interim analysis) • Appendices • Questionnaires • Consent forms • Instructions to interviewers
Example of a comparison table to demonstrate that randomization was successful
Incidence vs. Prevalence • In infectious diseases of short duration, incidence may be close to prevalence • In chronic diseases, prevalence will be far greater than incidence • Monitor disease burden by prevalence • Monitor efficacy of programs by incidence
Calculate an Incident Rate Jan July Jan July Jan July Jan July Jan July Jan time at 1976 1976 1977 1977 1978 1978 1979 1979 1980 1980 1981 risk Sub A *---------------------- 2.0 Sub B *---------------------------------x 3.0 Sub C *--------------------------------------------------------- 5.0 Sub D *--------------------------------------- 4.0 Sub E *---------------------------x 2.5 Total Years at risk 16.5 * = initiation of study ID=___cases/___person-years -- =Time followed x = development of disease
Measures of Associaton • Since clinical trials are prospective and the intervention precedes the outcome, a relative risk is calculated. • Covariates and confounders can be either controlled for in the design or adjusted for in the analysis
Is PID more common among HIV-infected women • Research Question • Population • Inclusion/exclusion • Study Design • Type of analysis and Unit of analysis • What are the predictors, confounders, and outcomes of interest • Findings • Limitations/Strengths
Difficulties with this study • Definition of a case • Choice a proper control • Detection bias
A microbicide to prevent HIV among women • Research Question • Population • Inclusion/exclusion • Study Design • Type of analysis and Unit of analysis • What are the predictors, confounders, and outcomes of interest • Findings • Limitations/Strengths
Difficulties with this study • Ethical dilemma • Exposure is altered by study itself • Choice of cases and controls • Sample size considerations
An HPV vaccine to prevent HPV among women • Research Question • Population • Inclusion/exclusion • Study Design • Type of analysis and Unit of analysis • What are the predictors, confounders, and outcomes of interest • Findings • Limitations/Strengths
Difficulties with this study • Misclassification bias possible • Population to study difficult to find • Sample size • Generalizability
Study Design • Statement of hypothesis • Population • Sampling • Inclusion/Exclusion • Time frame • Design • Measurement • Predictors • Confounders • outcome • Analysis plan • Sample size • Dummy Tables • Analyses to be done • Efforts to minimize threats to validity • Strengths and limitations