Download
1 / 15
150 likes | 257 Views
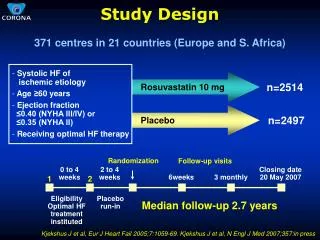
A Retrospective Study of Outcomes in Pediatric Hematology/Oncology Patients Receiving Continuous Venovenous Hemodialysis Y Avent 1 , N Henderson 1 , T Collie 1 , RF Tamburro 2 , L Elbahlawan 1 , RR Morrison 1 , S Rajasekaran 1 1 St. Jude Children’s Research Hospital, Memphis, TN

E N D
A Retrospective Study of Outcomes in Pediatric Hematology/Oncology Patients Receiving Continuous Venovenous Hemodialysis Y Avent1, N Henderson1, T Collie1, RF Tamburro2, L Elbahlawan1, RR Morrison1, S Rajasekaran1 1 St. Jude Children’s Research Hospital, Memphis, TN 2 Pennsylvania State University College of Medicine, Hershey, Pennsylvania
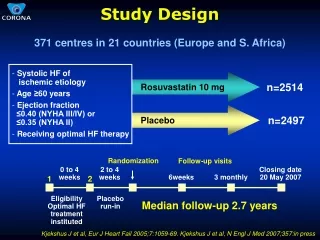
Study Design • Single Center Retrospective Review from January 2003-December 2007 • 8 bed ICU • Total CRRT days 689 averaging 172 treatment days/year • 41 patients received a total of 48 treatments • Median age of this cohort was 12 years. Range (7.8 months -24 years) • 23 males and 18 females • 30 Hematopoietic Stem Cell Transplant (HSCT) patients (73%) • Allogenic n=29 • Autologous n=1 • 11 non-HSCT patients (26%) • Acute Lymphoblastic Leukemia n=5 • Acute Myeloid Leukemia n=4 • Ewing’s Sarcoma n=1 • Glioblastoma Multiforme n=1
CRRT Modality • Modality • CVVHD • Anti-coagulant • Citrate • Dialysate • Normocarb HFTM • Dialysate rates • (2000ml/hr x BSA)/1.73m2=ml/hr • Blood Flow Rates • Average 2-4 ml/kg/min. • Filters • Renaflo II – polysulfone membrane • PAN – polyacrylonitrile membrane • Circuit Change • Every 3 days if patient’s clinical condition permits • Machine • B Braun Diapact
Indications for CRRT 41 patients with 48 episodes of CRRT • Fluid overload • n=12 • Renal Failure • acute: n=29 • transition from Intermittent Hemodialysis (IHD) to CRRT n=5 • Improving Fluid homeostasis in Congestive Heart Failure • n=1 • Tumor Cell Lysis • n=1
CRRT Variables • HSCT patients 15.9±2.02 days therapy • Non HSCT 9.6±2.9 days therapy • 2 different filters used ( PAN and Renaflo) • Of all variables statistically compared BUN > 75 at CVVHD initiation and C-Reactive Protein (CRP) at end of therapy were predictive of ICU death (p-value < 0.05). • Hyperglycemia, high creatinine, oliguria and fluid balance not predictive of ICU mortality. • A BUN > 29 mg/dL at day +7 was said to be predictive of mortality in HSCT patients in previous study. (Bacigalupo et al 1999)
CRRT Survivors • HSCT patients (n=30) • ICU survival – HSCT pts 36% • Reasons for CVVHD D/C • IHD Transition n=7 • Improved renal function n=4 • Support withdrawn n=2 • Non-HSCT patients (n=11) • ICU survival – non-HSCT pts 42% • Reasons for CVVHD D/C • IHD Transition n=2 • Improved Renal Function n=3
ICU Non-Survivors • HSCT ICU patients - 70% (21 of 30) • MSOD n=7 • Veno-occlusive disease of liver n=3 • Pulmonary failure n=3 • Sepsis n=2 • Cardiopulmonary failure n=2 • Relapse n=1 • Other n=3 • Median PRISM score at CRRT initiation n=17 • Non-HSCT patients – 55% (6 of 11) • MSOD n=3 • Primary malignancy n=2 • Secondary malignancy n=1 • Median PRISM score at CRRT initiation n=21.5
Survivors Vs Non Survivors * Non survivors had higher BUN at -24 * than survivors P<0.05.
HSCT patients * Difference in CRP value reaches statistical significance* only at CVVHD end
ICU Issues • HSCT patients - BUN > 75mg/dL and CRP are predictive of ICU mortality. • Mechanical ventilation, use of pressors, hyperglycemia at CVVHD onset not predictive of ICU mortality. • Oxygenation index and PF ratio in allogenic HSCT patients improved after 24 hours of CVVHD. • 13.2±1.5 Vs 9.2±1.5 and 176.7±17.2 Vs 236±20.3 (Both indices P<0.05) • Mean PRISM scores for CVVHD episodes among HSCT patients were 16.4±0.7 compared to non-HSCT 19.9±1.1 (not statistically significant)
6 month Survival • HSCT patients - 3% (1of 30 patients) • Only 3/30 HSCTs had recurrence of primary oncologic disease. • Non HSCT patients – 36% (4 of 11 patients) survived to 6 months • Overall 6 mo. Survival – 12% (5 of 41) • Benoit et al reported 6 month survival in adult patients with hematologic malignancies at 14%.
Limitations of Study • Small sample size makes it difficult to draw conclusions • Findings may not be relevant to other centers • Retrospective analysis • No data regarding patients not referred to the ICU for CRRT • Heterogeneity in primary oncologic disease and variation in oncologic therapy makes analysis difficult.
Conclusion • Effective, safe renal replacement modality • Resource intensive • Non-HSCT patient ICU survival compares favorably with general ICU populations (Goldstein et al Pediatrics 107(6); June 2001) • 6 month survival rates for HSCT patients is not encouraging
Ethical Considerations • Poor 6 month survival outcomes for HSCT patients • More selective in offering therapy if we can identify patients who are likely to survive to ICU discharge • Managing expectations of families
Future Research • Attempt to delineate factors which can translate short term success into 6 month survival for HSCT patients • Parent/patient perceptions • CVVHD vs. other modalities in HSCT patients • Immune modulation with CVVHD • PRISM scores for HSCT vs. Non HSCT patients