Download
1 / 58
581 likes | 806 Views
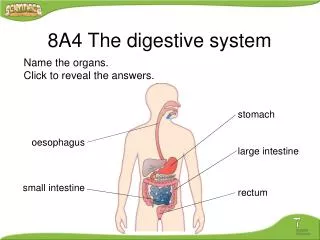
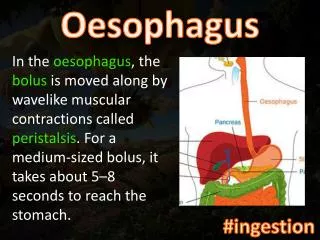
Oesophagus. Anatomical & physiological considerations. A muscular tube connecting pharynx to stomach. Guarded at both ends by sphincters. Lies anterior to cervical vertebrae in neck & in posterior mediastinum in chest & enters abdomen through oesophageal hiatus in diaphragm.

E N D
Anatomical & physiological considerations • A muscular tube connecting pharynx to stomach. • Guarded at both ends by sphincters. • Lies anterior to cervical vertebrae in neck & in posterior mediastinum in chest & enters abdomen through oesophageal hiatus in diaphragm. • The last 2-3 cm are within abdomen above GEJ with stomach. • The mucosal lining of oesophagus is pale grey & consists of squamous epithelium. • The musculature of upper two-thirds of oesophagus is striated & distal third is smooth. • The oesophagus is devoid of a serosal layer. Oesophagus
Anatomical and physiological considerations • The two sphincters are at the pharyngo-oesophageal junction (upper) & in the region of the oesophageal opening (hiatus) in the diaphragm. • Both have intrinsic & extrinsic components. Upper intrinsic sphincter • The main function of preventing access of air to the oesophagus & working in conjunction with laryngeal closure during swallowing. • It relaxes on initiation of the swallowing reflex • The superior constrictor extrinsic component contracts to expel food or liquid into oesophagus where a wave of peristalsis carries it downwards. Oesophagus
Anatomical and physiological considerations • Lower intrinsic sphincter is the circular smooth muscle of the oesophagus. • Its role is to prevent GE regurgitation & it is normally closed but relaxes in response to the swallowing wave. • The intrinsic sphincter is supplemented by the striated muscle of the right crus, which splits to embrace the lower end of the oesophagus (keeping GEJ closed when intra-abdominal pressure is significantly increased). • Another factor which prevents reflux from the stomach is the acute angle of insertion of the oesophagus into the stomach which brings the gastric and oesophageal walls in contact when intra-abdominal pressure rises. • Anatomical disorders at the diaphragmatic hiatus reduce the efficacy of the intrinsic sphincter. Oesophagus
Anatomical relationships of the oesophagus Oesophagus
Clinical features of oesophageal diseaseSymptoms Dysphagia • Difficulty in swallowing. Progressive • A malignant growth or a stricture reduces size of oesophageal lumen • Eventually goes on to total dysphagia when neither food, liquid nor the patient's own saliva can be swallowed. • High grades of dysphagia are often associated with regurgitation into pharynx & upper air passages & therefore with respiratory infection. Non-progressive • Disorders of function either of the whole oesophagus or at the lower sphincter. Oesophagus
Clinical features of oesophageal diseaseSymptoms Pain • Pain is ill-localised in chest (retrosternal). • May accompany partial dysphagia from obstruction. • It also occurs in motility disorders. • Confusion with pain originating in heart muscle is common. Heartburn • Heartburn is a retrosternal sensation of discomfort & burning. • Due to regurgitation from stomach into normally empty oesophagus. • If there is considerable reflux, patient may feels presence of liquid in pharynx. Oesophagus
Clinical features of oesophageal diseaseSigns • The deep situation of the oesophagus usually makes specific clinical features entirely absent. • May accompany individual disorders. Oesophagus
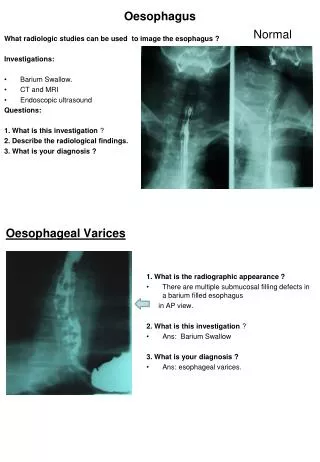
Investigation Radiology • Anteroposterior plain X-ray may occasionally show a broadening of the mediastinal shadow by a dilated oesophagus. • An air-fluid level may be seen behind the heart if there is distal oesophageal obstruction. • Contrast radiology, usually with barium sulphate but in special circumstances with a water-soluble contrast medium, is the standard method of establishing both anatomical & functional abnormality. Endoscopy • The flexible oesophago-gastroduodenoscope is now often used as an alternative or complement to contrast radiology to achieve a diagnosis & has the advantage of being able to take tissue for histological examination. Oesophagus
Investigation Manometry & oesophageal pH studies • Has an increasing role in the analysis of disorders of motility. • Similar equipment can be used for monitoring acid level in oesophagus in patients with suspected reflux. • The technique is to place a pH sensor at end of a tube in lower oesophagus & to make continuous recordings over 24 hours. • In normals there should be little change; however, in those with reflux of acid contents, the pH falls sporadically, particularly at night. Oesophagus
Motility disorders • Hypermotility – chiefly diffuse spasm • Hypomotility – usually secondary to systemic sclerosis (scleroderma) • Sphincter dysfunction – the inability of lower sphincter to relax (achalasia). Oesophagus - Motility disorders
HypermotilityDiffuse oesophageal spasm Aetiology • The cause is unknown (rare) Clinical features • Intermittent, severe chest pain with dysphagia. • DD angina pectoris. Investigation • A contrast study shows exaggerated oesophageal contractions (corkscrew). • Oesophagoscopy is usually normal, but manometry shows exaggerated contractions. Management • Drugs that reduce smooth muscle contraction (nitrates & calcium channel blockers such as nifedipine) occasionally help. • Balloon dilatation is also an option. • Long oesophageal myotomy in which all layers of muscle down to mucosa are divided may be required. Oesophagus - Motility disorders
HypermotilityNutcracker (super-squeeze) oesophagus • It is a common manometric finding in patients who present with chest pain which is of non-cardiac origin. • The symptoms are the same as those for diffuse spasm, as is the management. • However, surgical treatment is rarely required. Oesophagus - Motility disorders
Hypomotility Systemic sclerosis • Of unknown cause. • The muscle layer is replaced by fibrous tissue. • The presence of the disease may be suspected from other features such as loss of mobility of the face & microvascular features, e.g. digital ischaemia. Investigation and management • Contrast radiology shows diminished peristalsis & confirmed by manometry. • The treatment of hypomotility is that of the complications such as GER. Oesophagus - Motility disorders
Achalasia (cardiospasm) Aetiology • In the great majority of patients the cause is unknown, but a similar clinical condition is found in South America as a result of infection with a protozoan organism Trypanosoma cruzi. • The lower sphincter fails to relax in response to the peristaltic wave, & the bolus is partially retained in the oesophagus. Oesophagus - Achalasia
Achalasia Clinicopathological features • Dilatation and muscular hypertrophy occur above the lower sphincter. • Histological examination shows loss of ganglion cells. • In long-standing cases the oesophagus becomes elongated & inflamedmucosa from stasis of food ? → development of malignant change. • Initially no frank dysphagia but rather a slowing down of normal rate of ingestion of food. • Obvious dysphagia ultimately develops with retrosternal discomfort, regurgitation & weight loss. • Symptoms in later life may lead to confusion between achalasia & carcinoma. Oesophagus - Achalasia
Achalasia Investigation • Endoscopy is essential and in older patients may show a secondary cause such as infiltration of the distal oesophagus by malignant disease. • Contrast study confirms delay at the lower sphincter, although in early symptomatic patients the abnormality may be difficult to identify. • Manometry shows incomplete relaxation of lower sphincter in response to a swallow. Oesophagus - Achalasia
Achalasia Management • Balloon dilatation, which leads to resolution of symptoms in 80% although it may have to be repeated and carries a small risk of oesophageal perforation • Longitudinal myotomy of the gastro-oesophageal junction (Heller's operation) which can be done either at open operation or via a laparoscope or thoracoscope ± anti-reflux procedure. • Surgical myotomy is associated with a small risk of GER but is otherwise a very satisfactory procedure. • Endoscopic injection of botulinum toxin into oesophageal wall to paralyse LES. Oesophagus - Achalasia
Gastroesophageal reflux disorders • Features of reflux occur in association with many different oesophageal conditions, including most of the motility disturbances. • Reflux is particularly a symptom of abnormalities at the diaphragmatic hiatus. Oesophagus - Gastroesophageal reflux disorders
Gastroesophageal reflux disorders Pathophysiological features • If either acid or strongly alkaline secretions reach the lower oesophagus → mucosal inflammation. • Mostly a superficial oesophagitis. • Stricture – this is usually predominantly an inflammatory reaction in the mucosa & submucosa, but it can, if inflammation takes place, become a fibrous narrowing • Metaplastic change – this leads to development of gastric-type columnar epithelium in lower oesophagus ('Barrett's oesophagus‘). • It is a premalignant lesion (adenocarcinoma). Oesophagus - Gastroesophageal reflux disorders
Gastroesophageal reflux disorders Clinical syndromes Two main causes: • Hiatus hernia with reflux. • Reflux without abnormal anatomy. Oesophagus - Gastroesophageal reflux disorders
Hiatus hernia Types of hiatus hernia: • Sliding (usually associated with reflux) & paraesophageal. • Mixed (type III). Oesophagus - Hiatus hernia
(a) The esophagogastric anatomy in a sliding hiatus hernia.(b) The anatomy in a paraesophageal hernia. Hiatus hernia
Sliding hiatus hernia • The proximal stomach ascends into the chest through a lax or enlarged diaphragmatic opening, taking a circumferential cuff of peritoneum with it. • The normally acute oesophagogastric angle is reduced, so that reflux is common even though the intrinsic lower sphincter is normal. Aetiology • Obesity, increase in abdominal contents (pregnancy) & ageing may be contributory factors. Clinical features • There is postural reflux, heartburn & occasionally some lower left chest pain. • Vague indigestion is rarely caused by a sliding hernia. Oesophagus - Hiatus hernia
Sliding hiatus herniaInvestigation • Patients with the recent onset of symptoms, particularly if they are elderly, should be investigated for possible oesophagogastric cancer. Contrast radiography • The standard method of making the diagnosis is by barium swallow & meal. Endoscopy • Although it is not always easy to identify the esophagogastric junction, this examination allows assessment of severity of oesophagitis, & a tissue diagnosis by examination of a biopsy may be made in patients with Barrett's oesophagus. pH Monitoring • Oesophageal pH studies are useful in cases of diagnostic uncertainty and as a baseline measurement before surgical treatment. Oesophagus - Hiatus hernia
Sliding hiatus herniaManagement Medical measures for the control of reflux: • Weight loss in the obese • Sleeping with the head of the bed raised to avoid nocturnal reflux • Alginate-containing antacids which are thought to reduce free liquid in the stomach and thus reduce the volume of reflux • Acid reduction by H2-receptor antagonists (e.g. cimetidine or ranitidine) or proton pump inhibitors (e.g. omeprazole or lansoprazole). • If these measures fail to control symptoms or the patient is not keen on long-term medication, then operation should be considered. Oesophagus - Hiatus hernia
Sliding hiatus herniaManagement Surgical repair • May be carried out at open operation or at laparoscopy. • Reduction of the herniated stomach below the diaphragm • Removal of the circumferential peritoneal sac • Re-establishment of the esophagogastric angle reduction of the intercrural space by suturing the crura together behind the oesophagus an anti-reflux procedure-often loosely called a fundoplication. • The last procedure is increasingly used although it may not always be justified. The fundus of the stomach is wrapped around the terminal oesophagus so that, as intra-abdominal pressure rises, the oesophagus is compressed (Fig. 18.3). • Complication may be the inability to belch and bloating-a sensation of unrelieved fullness of the stomach. • Some patients experience postoperative dysphagia, which is usually transient. Oesophagus - Hiatus hernia
A fundoplication operationThe gastric fundus is wrapped around the abdominal esophagus Hiatus hernia
Hiatus herniaPara-oesophageal hernia Aetiology • A discrete peritoneal sac occurs at the left lateral border of oesophagus & fundus of stomach rolls into this, sometimes carrying the EGJ into the chest. • May cause a twist of the whole stomach-a gastric volvulus. Clinical features • Usually asymptomatic, although vague upper abdominal pain may occur. • Incarceration going on to strangulation is not common but causes acute upper abdominal pain → total dysphagia. • This occurrence - usually in elderly frail individuals - is a surgical emergency. Management • Unless the patient is unfit, paraesophageal hernias should be repaired surgically because of the risk of strangulation. Oesophagus - Hiatus hernia
Reflux without abnormal anatomy Aetiology and clinical features • Symptoms of reflux without any demonstrable anatomical abnormality. • In some, obesity is a factor; others may have hyperchlorhydria with or without a demonstrable peptic ulcer. • In the majority a definite cause is not identified. • Features of heartburn & dyspepsia, with regurgitation of gastric contents in some. Investigation • Treated symptomatically without investigation. • Those with troublesome features should have a barium swallow and endoscopy. • Ambulatory monitoring of lower oesophageal pH may establish that there is persistent reflux, and oesophageal manometry identifies those with a motility disorder. Management • Medical management. • Oesophagitis which is unresponsive to treatment, an anti-reflux operation should be considered but only after careful assessment of the benefit that is likely to be achieved. Oesophagus
Oesophageal diverticula • Hypopharyngeal pouch is the most common of these. • Other diverticula in lower parts of the oesophagus are rare. Oesophagus - Oesophageal diverticula
Oesophageal rupture & mucosal tear (Mallory-Weiss syndrome) Aetiology Aetiology • Vomiting is usually a coordinated event. The stomach and diaphragm contract so that intragastric pressure is raised; the oesophageal sphincters then relax, as does the oesophagus as a whole, and the stomach content is ejected. • However, this orderly course may not take place if: • Voluntary inhibition is necessary • Vomiting is artificially induced • The individual is confused – usually from excessive consumption of alcohol. • In such circumstances, intragastric pressure forces stomach contents into the distal oesophagus, dilating it. • The oesophagus may rupture with emptying of stomach contents into the left pleural cavity or, because the relatively elastic muscle has a greater capacity for stretch than does the folded mucosa and submucosa, only these are split to produce a longitudinal tear at the oesophagogastric junction. Oesophagus
Incomplete lower oesophageal tear (Mallory-Weiss syndrome) • The mechanism is the same as that for a complete tear. • The history is typically of an initial blood-free vomit followed by bright red haematemesis later. • Most episodes of bleeding from this cause are usually minor and self-limiting but are occasionally severe and persistent. • If this is the case, the stomach is exposed, opened and the tear oversewn, nearly always with good results. Acute upper-gastrointestinal bleeding
Oesophageal ruptureClinical features Clinical features History • Forceful vomiting may be with much intake of alcohol. • Vomiting may also have been induced either in a glutton or in someone who is mentally disturbed with a history of excessive eating but with the paradoxical desire not to gain weight (bulimia). • There will be sharp left-sided pleuritic pain. Physical findings • The effect of gastric content within the chest is to rapidly produce signs of severe sepsis with fever and circulatory disturbance. • A left pleural effusion is present. • The course is downhill with all the features of systemic inflammatory response syndrome. • Occasionally, however, the rupture is localised and the patient is less ill with localised pleural signs and features of sepsis which are less severe. Oesophagus - Oesophageal rupture
Oesophageal ruptureClinical features Management • In early rupture, the oesophagus is exposed and repaired. • Gastrostomy is often done to drain gastric secretions. • Parenteral or enteral (jejunostomy) nutrition is used until healing is assured. Oesophagus - Oesophageal rupture
Oesophageal ruptureMucosal tear Mucosal tear • The presentation of this condition is with haematemesis. Oesophagus - Oesophageal rupture
Cancer of the esophagusEpidemiology Epidemiology • This condition is relatively rare in the western world. • In the Far East the incidence is in general much higher (China). • Overall, the incidence is rising worldwide. Oesophagus - Cancer of the esophagus
Cancer of the esophagusAetiology Squamous carcinoma • The wide geographical variation in incidence has been attributed to social & environmental factors. • A strong association between cigarette & alcohol consumption & incidence of disease. • Diet is of greatest importance. Three factors are recognised: • High intake of nitrosamines derived from nitrates used in food preservatives • Low intake of both vitamin A & nicotinic acid • Iron deficiency anaemia, a known associate of hypopharyngeal cancer. • Long-standing achalasia may lead to cancer ? due to stasis & mucosal irritation. Oesophagus - Cancer of the esophagus
Cancer of the esophagusAetiology Adenocarcinoma • Cases of adenocarcinoma of the oesophagus now exceed those of squamous carcinoma in a ratio of 2:1. • Metaplastic change in the oesophageal mucosa from squamous to columnar epithelium as a result of reflux (Barrett's oesophagus) predisposes to development of adenocarcinoma. Oesophagus - Cancer of the esophagus
Cancer of the esophagusPathological features Pathological features • Nearly all lesions are a combination of narrowing & ulceration. Spread by: • direct invasion first through full thickness of oesophageal wall and then into adjacent structures such as the trachea or bronchi, the pericardium, chest wall and diaphragm. • submucosal infiltration both proximally & distally • lymph node involvement in the mediastinum and, in distal lesions, around the stomach. Upward spread in the mediastinum may produce a sentinel node in the supraclavicular fossa • the bloodstream - distant metastases (liver, lung and brain). Oesophagus - Cancer of the esophagus
Cancer of the esophagusClinical features Clinical features Symptoms • The mean duration of symptoms is 4-6 months but may be up to 3 years. Early ill-defined symptoms • There may be a feeling of something stuck in the oesophagus. • Retrosternal discomfort, belching & dyspepsia. Oesophagus - Cancer of the esophagus
Cancer of the esophagusClinical features Progressive dysphagia • The most common presenting symptom (2/3 of oesophageal diameter). • In the early stages, dysphagia is for solids only, later difficulty with liquids. • Regurgitation after eating • May be delay until dysphagia is total (inability to swallow saliva). Weight loss • More than 10-15% of the pre-illness weight may be lost over 4-6 weeks. Acute obstruction • Precipitated by the impaction of a large (inadequately chewed) food bolus. Oesophagus - Cancer of the esophagus
Cancer of the esophagusClinical features Miscellaneous • A long history of heartburn suggestive of acid reflux in patients with an adenocarcinoma in an area of columnar metaplasia. • Pain may indicate penetration of tumour outside wall of oesophagus. • Productive cough, particularly at night, due to aspiration of retained material into respiratory tract or by development of a malignant oesophagotracheal fistula. • Hoarseness may mean involvement of the recurrent laryngeal nerve. • Features of distant metastases can be the cause of presentation. Oesophagus - Cancer of the esophagus
Cancer of the esophagusClinical features Signs • Clinical examination of a patient with localised oesophageal cancer usually does not reveal any abnormalities other than evidence of recent weight loss. • Total dysphagia is associated with signs of lack of water - reduced skin turgor & a coated furred tongue. Signs of dissemination • Palpable lymphadenopathy, usually in supraclavicular region. • Hepatomegaly, jaundice, ascites, cardiac arrhythmias & features of pulmonary consolidation. • Respiratory infection due to aspiration of oesophageal content. Oesophagus - Cancer of the esophagus
Cancer of the esophagusInvestigation Investigation Radiography Barium swallow: • simplicity • relative lack of expense • high sensitivity in diagnosis of a stricture • accurate determination of the anatomical site • definition of the anatomy of the stomach & duodenum • creation of a 'road map' for endoscopy. Oesophagus - Cancer of the esophagus