Download
1 / 31
310 likes | 525 Views
Cardiac output = peripheral flow = AOP / peripheral resistance. Arterial volume = cardiac output - peripheral flow dt. AOP = arterial volume/arterial compliance.

E N D
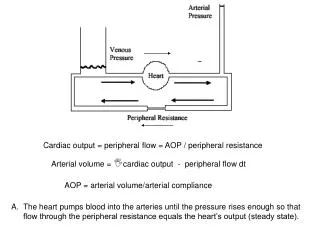
Cardiac output = peripheral flow = AOP / peripheral resistance Arterial volume = cardiac output - peripheral flow dt AOP = arterial volume/arterial compliance • The heart pumps blood into the arteries until the pressure rises enough so that flow through the peripheral resistance equals the heart’s output (steady state).
Because the blood volume is constant a fall in arterial pressure causes the arteries to recoil and moves blood volume from the arteries into the veins. This causes a rise in venous volume which raises the venous pressure. The veins are more compliant than the arteries. Thus a large fall in AOP causes a smaller rise in venous pressure (~10 :1).
Venous pressure is a major determinant of stroke volume in the heart. Thus a fall in arterial pressure raises venous pressure and acts to increase the cardiac output which restores the arterial pressure. This negative feedback makes the circulation quite stable.
Add 1 gm of dye Concentration is .01 gm/gal How big is the container? 100 gal The Fick Principle Measurement of Cardiac output clinically is done by indicator dilution methods.
The patient’s own oxygen is used as the indicator Vol % = cc of oxygen (STP) dissolved in 100 cc of blood
How many beakers pass under the spigot every minute? Each beaker represents 100 cc blood.
A more modern technique is the dye dilution method. ΔQ = [Q]t • Flow • Δt Q = [Q]t• Flow• Δt Q = Flow • [Q]t dt Flow = ∞ 0 Q [Q]t dt
In the common heart attack a thrombus forms in a coronary artery. Because heart muscle does not regenerate death of more than 1/3 of the left ventricle will lead to heart failure. Acute Myocardial Infarction
Acute Myocardial infarction • Symptoms are pain (usually in the chest), sweating and nausea • Heart muscle stops contracting seconds after its blood supply is lost (cessation of mechanical activity acts to conserve ATP). If the occluded artery is large it can put the heart into immediate failure • Heart muscle starts to die after about 20 min of ischemia. Treatment usually involves restoring flow by removing the clot. • Ventricular fibrillation (cardiac arrest with sudden death) may frequently occur. • 1. Blood pressure and organ perfusion falls to zero • 2. CPR is needed to keep the brain alive and to give enough coronary blood flow so that the heart can beat if the fibrillation is corrected. • 3. The defibrillator puts the entire heart into a refractory period so it can beat again.
Pressure overload causes concentric hypertrophy where the ventricle remodels inwardly to a low lumen volume and a thick wall. Caused by hypertension or outflow track obstruction.
Caused byregurgitant aortic valve or AV fistulas. Volume overload leads to eccentric hypertrophy. The heart remodels outwardly to give a large lumen volume and a thin wall
If the heart tries to compensate for an abnormal work load by hypertrophy it will end in failure. It is literally replacing good muscle with inferior muscle.
Cardiomyopathy: The heart muscle looses contractility for no apparent reason (idiopathic). • Common in the elderly • May be genetic (dilated cardiomyopathy) • Transplant
Post-infarction remodeling of the heart Myocardial infarction causes the surviving myocardium to hypertrophy as it takes over the work load.
In the failing heart contractility is reduced because of disease. The heart develops less pressure for any diastolic volume and as a result stroke volume is reduced.
Heart failure will cause arterial pressure to fall and venous pressure to rise.
The kidney will attempt to restore arterial pressure by retaining fluid and further raise venous pressure.
Shock is a condition where CO is not large enough to meet the requirements of the periphery. • Compensated stage: Reflexes maintain blood pressure. Recovery will occur unassisted. • B. Progressive stage: Reflexes eventually fail to maintain arterial pressure. The system deteriorates to death without intervention. • C. Irreversible Stage: The stage where irreversible injury has occurred to the system such that nothing will save the individual.
Septic Shock is a special case as cardiac output may be normal but still inadequate to meet the high metabolic requirements of the septic patient: • A. High fever • B. Maintained cardiac output in early stages • C. Disseminated intravascular coagulation as blood vessels deteriorate.
Irreversible shock: Failure to maintain peripheral resistance (necrosis of peripheral tissue), loss of endothelial barrier to plasma proteins causes edema with loss of blood volume into tissues. Endotoxin is released from bowel which widely dilates the blood vessels.
Hemorrhagic Shock (loss of Blood Volume) Blood volume is a major determinant of cardiac output
Decreasing total blood volume (or dilating the veins) will decrease cardiac output due to the decreased cardiac filling pressure.
Loss of peripheral tone reduces filling pressure: anaphylactic reaction, spinal chord injury, emotional shock, endotoxin
Causes of low cardiac output (continued). • Decreased output from the heart (cardiogenic): heart failure • 1. Coronary artery disease Acute myocardial infarction • 2. Other causes e.g. arrhythmia or tamponade • 3. End stage of chronic heart failure
It is erroneously believed that circulatory shock means low blood pressure. Although blood pressure will fall in the end-stages it is often normal in the early stages and is an unreliable index of inadequate cardiac output. More reliable signs are: • Pale mucous membranes, pale skin and finger nails • Cold skin • Narrow pulse pressure, tachycardia • Low urine production • Thirst • Confusion (cerebral ischemia)