Download
1 / 26
300 likes | 856 Views
Nicotine Dependence. Laurie Zawertailo, PhD Adjunct Research Scientist Clinical Neuroscience, CAMH. Objectives. To review the main physiological and pharmacological aspects of nicotine use, abuse, and dependence. To discuss the different treatments available for nicotine dependence.

E N D
Nicotine Dependence Laurie Zawertailo, PhD Adjunct Research Scientist Clinical Neuroscience, CAMH
Objectives • To review the main physiological and pharmacological aspects of nicotine use, abuse, and dependence. • To discuss the different treatments available for nicotine dependence.
Cigarette Smoking (Statistics) • 47% worldwide • 47% men • 12% women • 25% North America • 1/3 - 1/2 of adolescents daily smoking • 15% - 25% success rate to quit smoking • Spontaneous quit rates in adults 6-7%
Costs of Tobacco Dependence • 30% (males) and 17% (females) of all cancer deaths in Canada are due to smoking. • Over 25% of cancer burden in Canada is attributable to lung cancer. • 80 - 90% of lung cancers are directly attributable to smoking • Smoking is also directly linked to • Diabetes • Heart disease • Stroke • Respiratory diseases • CV disease
Factors Associated With Smoking • Biological hereditary, psychiatric, psychological • Environmental parties, bars • Social predisposition family, friends, cultural • Easy access • Socially acceptable? • Peer pressure
Factors ENVIRONMENT VECTOR HOST AGENT
Release of catecholamines increasing sympathetic tone (GI motility, cardiac stimulation), arginine-vasopressin, beta endorphins, ACTH, cortisol, GH, PL, etc. • Enhanced memory, task performance, concentration, attention, and anxiety reduction. ?
Clinical conditions associated with smoking: • Respiratory • Cardiovascular Comorbidity: • Psychiatric disorders Schizophrenia, depression, anxiety • Other drugs of abuse Alcohol abuse/dependence
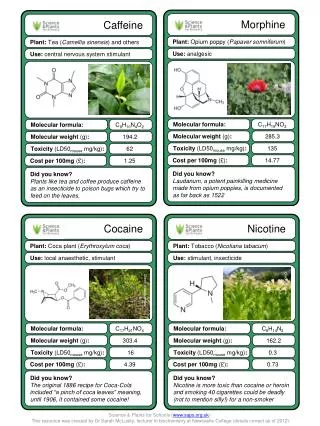
Nicotine • Psychoactive drug contained in tobacco • Likely responsible for the addictive properties of cigarettes • Self-administered by animals and humans • Reinforcing and rewarding • Following continuous administration the reinforcing effects of nicotine become prominent and the control over its use is lost
Nicotine content in cigarettes: 6 – 11 mg (1-3 mg are absorbed) Pack a day = 20 – 40mg Smokers adjust their nicotine intake High yield nicotine – less cigarettes Low yield nicotine – more cigarettes
Pharmacology of Nicotine Absorption • Buccal and nasal mucosa, skin, GI tract • Blood flow, membrane permeability, surface area, and pH Other factors known to modify the rate of absorption: • Degree and depth of inhalation • Number, duration, and volume of puffs • Use of a filter • Number of cigarettes smoked • Time spent smoking each cigarette
Peak nicotine concentrations are reached after completion of cigarette smoking Distribution • 19 seconds to reach the brain • Half-life: 2 hours Metabolism and elimination Liver and kidneys Main metabolite: cotinine (70% - 80%) CYP 2A6
Neuropharmacology of Nicotine Dependence • nAChR’s • Dopaminergic system (reward) • Tolerance, physical dependence • MAO A and B
Cigarette Smoking initiation Nicotine Smoking continuation Reward Pathological learning Active nAChRs Dopamine release Desensitized nAChRs Acute tolerance Inactive nAChRs Chronic tolerance Perpetuation of smoking behaviour Smoking discontinuation Hyper excitable nAChRs Withdrawal Increased no. of AChRs Smoking relapse Drive for the next cigarette
Tobacco as a Drug of Abuse Goodman and Gilman, 2001
Psychological Irritability Anxiety Aggressiveness Inability to concentrate Depressed mood Physical Difficulty sleeping Increased appetite Headache Nicotine Withdrawal Syndrome
Drug (Nicotine) DependenceDSM IV Criteria • Inability to stop using the drug • Preoccupation about drug use • Use despite harmful consequences • Presence of symptoms accounting for brain adaptation resulting in persistence use of the drug • Use despite significant drug-related problems
Treatments for Nicotine Dependence Behavioural Intervention Therapies Individual behavioural counseling Nicotine fading Aversion treatments Acupuncture Hypnosis
Nicotine Replacement Therapies Patch (7, 14, 21, 22mg) 6-12 wks Gum (2 and 4mg) 8-12 wks Inhaler (4mg/cartridge) 6 – 16/day 3-6 mo Nasal spray (1-2/hr; 0.5mg each; max 40mg/day) 3-6mo Low yield cigarettes
Bupropion 150mg twice/day 8-12 wks Risk of seizures (>300mg) Nortriptyline Clonidine Nicotine Blockade Therapy Mecamylamine Experimental approaches GABA agonists (vigabatrin)
Factors Associated With Low Quitting Success Rate • Comorbid psychiatric conditions • Alcohol or substance abuse • High nicotine dependence • Lack of social support for quitting • Low self-confidence in ability to quit
Treating Tobacco Dependence • Smoking is a complex human behaviour • Often takes several quit attempts before one is successful • NRT is most successful when combined with supportive care. • Lapse and relapse is very common.