Download
1 / 1
10 likes | 102 Views
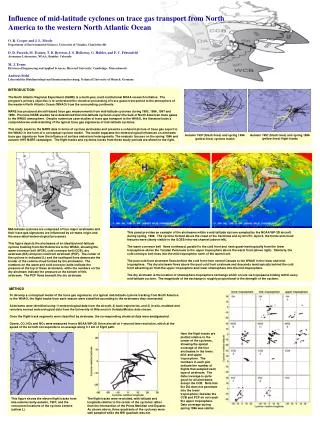
Differential Processing of Emotional Cues in Inpatients and Outpatients with Serious Mental Illness Melissa Tarasenko, Petra Kleinlein, Kee-Hong Choi, Elizabeth Cook, Charlie A. Davidson, and William D. Spaulding University of Nebraska-Lincoln.

E N D
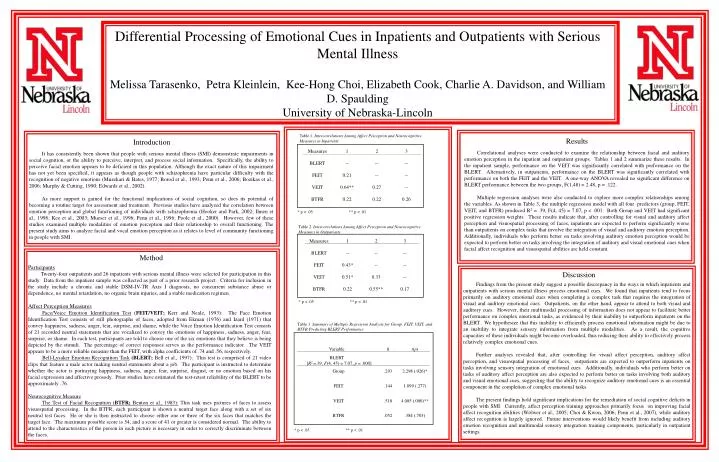
Differential Processing of Emotional Cues in Inpatients and Outpatients with Serious Mental Illness Melissa Tarasenko, Petra Kleinlein, Kee-Hong Choi, Elizabeth Cook, Charlie A. Davidson, and William D. Spaulding University of Nebraska-Lincoln Table 1. Intercorrelations Among Affect Perception and Neurocognitive Measures in Inpatients Results Introduction Correlational analyses were conducted to examine the relationship between facial and auditory emotion perception in the inpatient and outpatient groups. Tables 1 and 2 summarize these results. In the inpatient sample, performance on the VEIT was significantly correlated with performance on the BLERT. Alternatively, in outpatients, performance on the BLERT was significantly correlated with performance on both the FEIT and the VEIT. A one-way ANOVA revealed no significant difference on BLERT performance between the two groups, F(1,48) = 2.48, p = .122. Multiple regression analyses were also conducted to explore more complex relationships among the variables. As shown in Table 3, the multiple regression model with all four predictors (group, FEIT, VEIT, and BTFR) produced R2 = .39, F(4, 45) = 7.07, p < .001. Both Group and VEIT had significant positive regression weights. These results indicate that, after controlling for visual and auditory affect perception and visuospatial processing of faces, inpatients are expected to perform significantly worse than outpatients on complex tasks that involve the integration of visual and auditory emotion perception. Additionally, individuals who perform better on tasks involving auditory emotion perception would be expected to perform better on tasks involving the integration of auditory and visual emotional cues when facial affect recognition and visuospatial abilities are held constant. It has consistently been shown that people with serious mental illness (SMI) demonstrate impairments in social cognition, or the ability to perceive, interpret, and process social information. Specifically, the ability to perceive facial emotion appears to be deficient in this population. Although the exact nature of this impairment has not yet been specified, it appears as though people with schizophrenia have particular difficulty with the recognition of negative emotions (Muzekari & Bates, 1977; Borod et al., 1993; Penn et al., 2006; Bozikas et al., 2006; Murphy & Cutting, 1990; Edwards et al., 2002). As more support is gained for the functional implications of social cognition, so does its potential of becoming a routine target for assessment and treatment. Previous studies have analyzed the correlation between emotion perception and global functioning of individuals with schizophrenia (Hooker and Park, 2002; Ihnen et al., 1998; Kee et al., 2003; Mueser et al., 1996; Penn et al., 1996; Poole et al., 2000). However, few of these studies examined multiple modalities of emotion perception and their relationship to overall functioning. The present study aims to analyze facial and vocal emotion perception as it relates to level of community functioning in people with SMI. * p < .05 ** p < .01 Table 2. Intercorrelations Among Affect Perception and Neurocognitive Measures in Outpatients Method Participants Twenty-four outpatients and 26 inpatients with serious mental illness were selected for participation in this study. Data from the inpatient sample was collected as part of a prior research project. Criteria for inclusion in the study include a chronic and stable DSM-IV-TR Axis I diagnosis, no concurrent substance abuse or dependence, no mental retardation, no organic brain injuries, and a stable medication regimen. Affect Perception Measures Face/Voice Emotion Identification Test (FEIT/VEIT; Kerr and Neale, 1993): The Face Emotion Identification Test consists of still photographs of faces, adopted from Ekman (1976) and Izard (1971) that convey happiness, sadness, anger, fear, surprise, and shame, while the Voice Emotion Identification Test consists of 21 recorded neutral statements that are vocalized to convey the emotions of happiness, sadness, anger, fear, surprise, or shame. In each test, participants are told to choose one of the six emotions that they believe is being depicted by the stimuli. The percentage of correct responses serves as the performance indicator. The VEIT appears to be a more reliable measure than the FEIT, with alpha coefficients of .74 and .56, respectively. Bell-Lysaker Emotion Recognition Task(BLERT; Bell et al., 1997): This test is comprised of 21 video clips that feature a male actor making neutral statements about a job. The participant is instructed to determine whether the actor is portraying happiness, sadness, anger, fear, surprise, disgust, or no emotion based on his facial expression and affective prosody. Prior studies have estimated the test-retest reliability of the BLERT to be approximately .76. Neurocognitive Measure The Test of Facial Recognition (BTFR; Benton et al., 1983): This task uses pictures of faces to assess visuospatial processing. In the BTFR, each participant is shown a neutral target face along with a set of six neutral test faces. He or she is then instructed to choose either one or three of the six faces that matches the target face. The maximum possible score is 54, and a score of 41 or greater is considered normal. The ability to attend to the characteristics of the person in each picture is necessary in order to correctly discriminate between the faces. Discussion Findings from the present study suggest a possible discrepancy in the ways in which inpatients and outpatients with serious mental illness process emotional cues. We found that inpatients tend to focus primarily on auditory emotional cues when completing a complex task that requires the integration of visual and auditory emotional cues. Outpatients, on the other hand, appear to attend to both visual and auditory cues. However, their multimodal processing of information does not appear to facilitate better performance on complex emotional tasks, as evidenced by their inability to outperform inpatients on the BLERT. We hypothesize that this inability to efficiently process emotional information might be due to an inability to integrate sensory information from multiple modalities. As a result, the cognitive capacities of these individuals might become overloaded, thus reducing their ability to effectively process relatively complex emotional cues. Further analyses revealed that, after controlling for visual affect perception, auditory affect perception, and visuospatial processing of faces, outpatients are expected to outperform inpatients on tasks involving sensory integration of emotional cues. Additionally, individuals who perform better on tasks of auditory affect perception are also expected to perform better on tasks involving both auditory and visual emotional cues, suggesting that the ability to recognize auditory emotional cues is an essential component in the completion of complex emotional tasks. The present findings hold significant implications for the remediation of social cognitive deficits in people with SMI. Currently, affect perception training approaches primarily focus on improving facial affect recognition abilities (Wölwer et al., 2005; Choi & Kwon, 2006; Penn et al., 2007), while auditory affect recognition is largely ignored. Future interventions would likely benefit from including auditory emotion recognition and multimodal sensory integration training components, particularly in outpatient settings. * p < .05 ** p < .01 Table 3. Summary of Multiple Regression Analysis for Group, FEIT, VEIT, and BTFR Predicting BLERT Performance * p < .05 ** p < .01