Download
1 / 51
570 likes | 914 Views
Introduction to leukemia. Acute leukemias. Introduction to leukemia. Leukemia is a malignant disease characterized by unregulated proliferation of one cell type. It may involve any of the cell lines or a stem cell common to several cell lines. Leukemias are classified into 2 major groups

E N D
Introduction to leukemia Acute leukemias
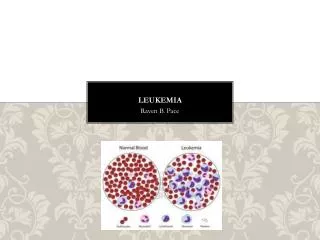
Introduction to leukemia • Leukemia is a malignant disease characterized by unregulated proliferation of one cell type. • It may involve any of the cell lines or a stem cell common to several cell lines. • Leukemias are classified into 2 major groups • Chronic in which the onset is insidious, the disease is usually less aggressive, and the cells involved are usually more mature cells • Acute in which the onset is usually rapid, the disease is very aggressive, and the cells involved are usually poorly differentiated with many blasts.
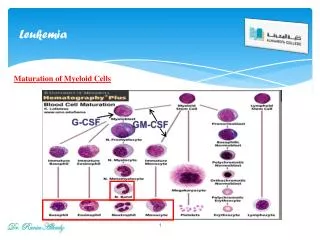
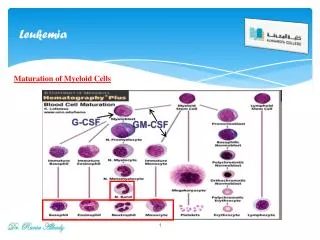
Introduction to leukemia • Both acute and chronic leukemias are further classified according to the prominent cell line involved in the expansion: • If the prominent cell line is of the myeloid series it is a myelocytic leukemia (sometimes also called granulocytic) • If the prominent cell line is of the lymphoid series it is a lymphocytic leukemia • Therefore, there are four basic types of leukemia • Acute myelocytic leukemia – AML- (includes myeloblastic, promyelocytic, monocytic, myelomonocytic, erythrocytic, and megakaryocytic) • Acute lymphocytic leukemia – ALL- (includes T cell, B cell, and Null cell) • Chronic myelocytic leukemia – CML - (includes myelocytic and myelomonocytic)
Introduction to leukemia • Chronic lymphocytic leukemia – CLL - (includes plasmocytic {multiple myeloma}, Hairy cell, prolymphocytic, large granular cell lymphocytic, Sezary’s syndrome, and circulating lymphoma) • Etiology – the exact cause is frequently notknown, but predisposing factors are known: • Host factors • Some individuals have an inherited increased predisposition to develop leukemia • There is an increased incidence in those with an inherited tendency for chromosome fragility or abnormality or those with increased numbers of chromosomes (such as Down’s syndrome). • Many of these diseases are characterized by chromosomal translocations.
Introduction to leukemia • There is an increased incidence in those with hereditary immunodeficiencies. • There is an increased incidence in those with chronic marrow dysfunction such as those with myeloproliferative diseases, myelodysplastic syndromes, aplastic anemia, or paroxsymal nocturnal hemoglobinuria. • Environmental factors: • Exposure to ionizing radiation • Exposure to mutagenic chemicals and drugs • Viral infections
Introduction to leukemia • Incidence • Acute leukemias can occur in all age groups • ALL is more common in children • AML is more common in adults • Chronic leukemias are usually a disease of adults • CLL is extremely rare in children and unusual before the age of 40 • CML has a peak age of 30-50
Introduction to leukemia • Comparison of acute and chronic leukemias: AcuteChronic Age all ages usually adults Clinical onset sudden insidious Course (untreated) 6 mo. or less 2-6 years Leukemic cells immature >30% blasts more mature cells Anemia prominent mild Thrombocytopenia prominent mild WBC count variable increased Lymphadenopathy mild present;often prominent Splenomegaly mild present;often prominent
Introduction to leukemia • Acute leukemia – • Is a result of: • Malignant transformation of a stem cell leading to unregulated proliferation and • Arrest in maturation at the primitive blast stage. Remember that a blast is the most immature cell that can be recognized as committed to a particular cell line. • Clinical features • Leukemic proliferation, accumulation, and invasion of normal tissues, including the liver, spleen, lymph nodes, central nervous system, and skin, cause lesions ranging from rashes to tumors. • A humoral mediator from the leukemic cells may inhibit proliferation of normal cells.
Introduction to leukemia • Failure of the bone marrow and normal hematopoiesis may result in pancytopenia with death from hemorrhaging and infections. • Lab evaluation • The lab diagnosis is based on two things • Finding a significant increase in the number of immature cells in the bone marrow including blasts, promyelocytes, promonocytes (>30% blasts is diagnostic) • Identification of the cell lineage of the leukemic cells
Introduction to leukemia • Peripheral blood: • Anemia (normochromic, normocytic) • Decreased platlets • Variable WBC count • The degree of peripheral blood involvement determines classification: • Leukemic – increased WBCs due to blasts • Subleukemic – blasts without increased WBCs • Aleukemic – decreased WBCs with no blasts • Classification of the immature cells involved may be done by:
Introduction to leukemia • Morphology – an experienced morphologist can look at the size of the blast, the amount of cytoplasm, the nuclear chromatin pattern, the presence of nucleoli and the presence of auer rods (are a pink staining, splinter shaped inclusion due to a rod shaped alignment of primary granules found only in myeloproliferative processes) to identify the blast type: • AML – the myeloblast is a large blast with a moderate amount of cytoplasm, fine lacey chromatin, and prominent nucleoli. 10-40% of myeloblasts contain auer rods.
Introduction to leukemia • ALL – in contrast to the myeloblast, the lymphoblast is a small blast with scant cytoplasm, dense chromatin, indistinct nucleoli, and no auer rods
Introduction to leukemia • Cytochemistry – help to classify the lineage of a leukemic cell (myeloid versus lymphoid) • Myeloperoxidase – is found in the primary granules of granulocytic cells starting at the late blast stage. Monocytes may be weakly positive.
Sudan black • Sudan black stains phospholipids, neutral fats and sterols found in primary and secondary granules of granulocytic cells and to a lesser extent in monocytic lysosomes. Rare positives occur in lymphoid cells
Nonspecific Esterase • Nonspecific esterase – is used to identify monocytic cells which are diffusely positive. T lymphocytes may have focal staining
Acid phosphatase • Acid phosphatase may be found in myeloblasts and lymphoblasts. T lymphocytes have a high level of acid phosphatase and this can be used to help make a diagnosis of acute T-lymphocytic leukemia.
Leukocyte Alkaline phosphatase • Leukocyte alkaline phosphatase – is located in the secondary granules of segmented neutrophils, bands and metamyelocytes. The LAP score is determined by counting 100 mature neutrophils and bands. Each cell is graded from 0 to 5. The total LAP score is calculated by adding up the scores for each cell.
Introduction to leukemia • Immunologic markers (immunophenotyping) – these are used mainly for lymphocytes, i.e., for determining B cell or T cell lineage. These tests rely on antibodies made against specific surface markers. • They constitute what we would call the primary antibody and in an indirect assay they are allowed to react with the cells and unbound antibody is then washed away. • Fluorescently labeled antibody (secondary antibody) against the primary antibody is added and allowed to react and then unbound secondary antibody is washed away. • The cells are then sent through a flow cytometer that will determine the number of cells that have a fluorescent tag and which are thus positive for the presence of the surface marker to which the primary antibody was made. • In a direct assay, the primary antibody is fluorescently labeled.
Direct versus indirect labeling of antigens B or T cell specific Ab B or T cell specific Ab B or T Cell marker B or T Cell marker
Terminal deoyxtidyl transferase • This is a unique DNA polymerase present in stem cells and in precursor B and T lymphoid cells. • High levels are found in 90% of lymphoblastic leukemias. • It can also be detected using appropriate antibodies and flow cytometry.
Introduction to leukemia • Cytogenetics – cytogenetics studies can now be used for diagnosis and for prognosis of hematologic malignancies. • Many leukemias (and lymphomas) are characterized by specific chromosomal abnormalities, including specific translocations and aneuploidy. The specific type of malignancy can be identified based on the specific abnormality or translocation. These may be identified by • Looking at the karyotypes of the chromsomes from the abnormal cells • DNA based tests – these tests are very useful for following the course of the disease • RT-PCR • Southern blotting • A normal karyotype is usually associated with a better prognosis.
Acute leukemias • Acute lymphoblastic leukemia – • They may be classified on the basis of the cytological features of the lymphoblasts into; • L1 - This is the most common form found in children and it has the best prognosis. • The cell size is small with fine or clumped homogenous nuclear chromatin and absent or indistinct nucleoli. • The nuclear shape is regular, occasionally clefting or indented. • The cytoplasm is scant, with slight to moderate basophilia and variable vacuoles. • L2 – This is the most frequent ALL found in adults. • The cell size is large and heterogenous with variable nuclear chromatin and prominent nucleoli. • The nucleus is irregular, clefting and indented. • The cytoplasm is variable and often moderate to abundant with variable basophilia and variable vacuoles.
Acute leukemias • L3 – This is the rarest form of ALL. • The cell size is large, with fine, homogenous nuclear chromatin containing prominent nucleoli. • The nucleus is regular oval to round. • The cytoplasm is moderately abundant and is deeply basophilic and vacuolated.
Acute leukemias • ALL may also be classified on the basis of immunologic markers into: • Early pre-B ALL • Pre-B ALL • B ALL • T ALL • Null or unclassified ALL (U ALL) - lack B or T markers and may be the committed lymphoid stem cell)
Acute leukemias • Incidence – ALL is primarily a disease of young children (2-5 years), but it can also occur in adults • Clinical findings – pancytopenia with resulting fatigue, pallor, fever, weight loss, irritability, anorexia, infection, bleeding, and bone pain. • L1 occurs in children, L2 in adults, and L3 is called Burkitts leukemia
Acute leukemias • Prognosis – age, WBC count, and cell type are the most important prognostic indicators • Patients younger then 1 and greater than 13 have a poor prognosis • If the WBC count is < 10 x 109/L at presentation, the prognosis is good; If the WBC count is > 20 x 109/L at presentation the prognosis is poor • T cell ALL (more common in males) has a poorer prognosis than any of the B cell ALLs which have a cure rate of 70%
Acute leukemias • Acute leukemias with mixed lineage – occasionally there are acute leukemias that are biphenotypic and display phenotypes for two different lineages • B lymphoid/myeloid • T lymphoid/myeloid • B/T lymphoid • Myeloid/Natural killer • A rare trilineage leukemia has also been seen (was B/T lymphoid/myeloid!)
Acute leukemias • Acute myeloid leukemia (also called acute granulocytic leukemia) – classification depends upon • Bone marrow blast morphology • Degree of cell maturation • Cytochemical stains • Immunophenotyping • AML is divided into 7 different classifications: • M1 – myeloblastic without maturation • The bone marrow shows 90% blasts and < 10% promyelocytes • The disease occurs in older adults
AML – M1 • Note the myeloblasts and the auer rod:
Acute leukemias • M2 – myeloblastic with maturation • The bone marrow shows 30-89% blasts and > 10% promyelocytes; • This is characterized by an 8,21 chromosomal translocation • This occurs in older adults • M3 – hypergranular promyelocytic • This form of AML has a bone marrow with >30% blasts • Is more virulent than other forms • Occurs with a medium age of 39 • The WBC count is decreased • Treatment causes a release of the granules and may send the patient into disseminated intravascular coagulation and subsequent bleeding • It is characterized by a 15,17 chromosomal translocation
AML – M2 • Note myeloblasts and hypogranulated PMNs:
AML – M3 • Note hypergranular promyelocytes:
Acute leukemias • M3m – hypogranular promyelocytic – • The bone marrow has > 30% blasts • The WBC count is increased. • Like the M3 type, treatment causes a release of the granules and may send the patient into disseminated intravascular coagulation and subsequent bleeding and • It is characterized by a 15,17 translocation • M4 – acute myelomonoblastic leukemia • Both myeloblasts and monoblasts are seen in the bone marrow and peripheral blood • Infiltration of extramedullary sites is more common than with the pure granulocytic variants
AML – M3M • Note hypogranular promyelocytes:
AML – M4 • Note monoblasts and promonocytes:
Acute leukemias • M5 – acute monoblastic leukemia • >80% of the nonerythroid cells in the bone marrow are monocytic • There is extensive infiltration of the gums, CNS, lymph nodes and extramedullary sites • This form is further divided into • M5A - Poorly differentiated (>80% monoblasts) • M5B - Well differentiated (<80% monoblasts) • M6 – erythroleukemia • This is rare and is characterized by a bone marrow having a predominance of erythroblasts • It has 3 sequentially morphologically defined phases; • Preponderance of abnormal erythroblasts • Erythroleukemia – there is an increase in both erythroblasts and myeloblasts • Myeloblastic leukemia – M1, M2, or M4 • Anemia is common
AML – M5A • Note monoblasts:
AML-M5B • Note monoblasts, promonocytes, and monocytes:
AML – M6 • Note M1 type monoblasts
Acute leukemias • M7 - Acute megkaryoblastic leukemia • This is a rare disorder characterized by extensive proliferation of megakaryoblasts, atypical megakaryocytes and thrombocytopenia • Treatment of leukemias – • There are 2 goals: • Eradicate the leukemic cell mass • Give supportive care • Except for ALL in children, cures are not common but complete remission (absence of any leukemia related signs and symptoms and return of bone marrow and peripheral blood values to within normal values) is