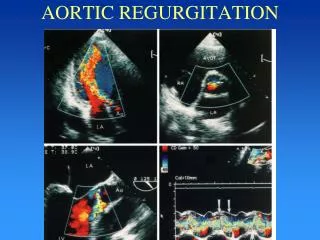
aortic regurgitation
200 likes | 947 Views
Pathophysiology. Chronic AR: LV overload ? LV dilatation, eccentric hypertrophy, insidious prog to CHF (decades, typically)Acute AR: nl LV poorly tolerates sudden increase LVEDV ? massive increase LVEDP leading to pulm edema, hypotension /- cardiogenic shock. Epidemiology. Overall prevalence 4.9%; moderate or greater severity 0.5% (Framingham)No sex or racial predilectionAge: dependent on etiology.

aortic regurgitation
E N D
Presentation Transcript
1. Aortic Regurgitation Dave Fitzhugh, MD
UNC Morning Report
March 21, 2008
2. Pathophysiology Chronic AR: LV overload ? LV dilatation, eccentric hypertrophy, insidious prog to CHF (decades, typically)
Acute AR: nl LV poorly tolerates sudden increase LVEDV ? massive increase LVEDP leading to pulm edema, hypotension +/- cardiogenic shock
3. Epidemiology
Overall prevalence 4.9%; moderate or greater severity 0.5% (Framingham)
No sex or racial predilection
Age: dependent on etiology
4. Etiology, Acute Infective endocarditis
Ascending dissection (type A)
Prosthetic valve dysfunction
Chest trauma
5. Etiology, Chronic Valvular
RHD (no longer common in US)
Bicuspid AoV
Infective endocarditis
Aortic root dz
CT dz: Marfan, Ehlers-Danlos, syphilis
Inflamm: Ankylosing spondylitis, Takayasu, RA, SLE
6. AR and Ankylosing Spondylitis 2-10% prevalence of symptomatic AR in AS (subclinically as high as 82% in TEE study of AS pts)
Similar prevalence in other HLA-B27 (Reiter�s, psoriatic arthritis, IBD-assoc arthritis)
Path involves aortic root/valve cusp retraction
Frequently have conduction disorders, including high grade AV block due to dz extension into septum
7. Clinical Manifestations Typically, classic CHF symptoms: DOE, orthop, PND
Often, palpitations 2/2 hyperdynamic LV. Rarely, syncope
Acute AR: pulm edema, hypotension prog to cardiogenic shock
8. Physical Exam Tachycardia, widened pulse pressure (though not in severe AR due to rapid equalization)
Murmur: classically, decrescendo diastolic murmur at LUSB (often unimpressive). Often, SEM with overloaded LV in mod to severe AR.
Diastolic �rumble� = Austin-Flint murmur, 2/2 regurg jet interacting with flow across mitral valve
S3 gallop
Murmur increased with sitting up, expiration (incr preload) and decreased with straining, valsalva
9. Fun you can have with eponyms! Corrigan�s pulse � water hammer pulse
de Musset sign - patient�s head bobs with each heartbeat
Quincke sign � subungual capillary pulsations
M�ller sign is systolic pulsations of the uvula
Traube sign � double sound over fem art with distal compression
Final Jeopardy: Landolfi�s sign = alternating constriction/dilatation of pupils
10. Differential Dx CHF
Other valvular lesions: AS, MS
Causes of AI as above: bicuspid valve, RHD, endocarditis, Marfan�s, HLA-B27, etc.
11. Diagnosis EKG typically with LVH, LAD, often left atrial enlargement
CXR: CM, sometimes root dilatation
TTE: estimate severity based on color flow dopplers
12. Severity Classification
13. TTE Before AVR
14. TTE After AVR
15. Treatment Medical
Afterload reduction: ACEI, nifedipine, hydralazine
Use BB cautiously, if at all, given prolonged diastole and therefore ? regurg volume
Surgical
AVR � 4% mortality alone, 6.8% with CABG
LV dysfunction often irreversible, despite AVR
16. Indications for AVR
17. Outcomes of AVR for AR 3/5/10 year survival regardless of EF: 82%, 76%, 67%
Improved somewhat with nifedipine preop in low EF (<35%) pts
Again, many times, LV dysfunction is irreversible despite AVR, so still need aggressive CHF regimen
18. References Enriquez-Sarano et al. Aortic Regurgitation. NEJM: 2004: (15); 1539-1546.
Huffer LL et al. Aortic root dilatation with sinus of valsalva and coronary artery aneurysms associated with ankylosing spondylitis. Tex Heart Inst J. 2006;33(1):70-3.
Hupppertz et al. Cardiac manifestations in patients with HLA B27-associated juvenile arthritis. Pediatr Cardiol. 2000 Mar-Apr;21(2):141-7.
19. The End