Download
1 / 41
560 likes | 1.57k Views
Echo Conference Aortic Regurgitation. September, 2007 Christopher Dibble, M.D. Aortic Regurgitation: Symptoms. Dyspnea, orthopnea, PND Chest pain. Nocturnal angina >> exertional angina (  diastolic aortic pressure and increased LVEDP thus  coronary artery diastolic flow)

E N D
Echo ConferenceAortic Regurgitation September, 2007 Christopher Dibble, M.D.
Aortic Regurgitation:Symptoms • Dyspnea, orthopnea, PND • Chest pain. • Nocturnal angina >> exertional angina • ( diastolic aortic pressure and increased LVEDP thus coronary artery diastolic flow) • With extreme reductions in diastolic pressures (e.g. < 40) may see angina
Quincke’s sign: capillary pulsation Corrigan’s sign: water hammer pulse Bisferiens pulse (AS/AR > AR) De Musset’s sign: systolic head bobbing Mueller’s sign: systolic pulsation of uvula Durosier’s sign: femoral retrograde bruits Traube’s sign: pistol shot femorals Hill’s sign:BP Lower extremity >BP Upper extremity by > 20 mm Hg - mild AR > 40 mm Hg – mod AR > 60 mm Hg – severe AR Peripheral Signs of Severe Aortic Regurgitation
Aortic Regurgitation • Can be a caused by: • Valve Disease • Aortic root disease • Percentage of aortic root disease steadily increasing over past few decades • Root disease now accounts for >50% of all AVRs
AR – Valvular disease • Rheumatic disease • Cusps become fibrotic and retract • Usually also stenotic • MV is involved • Calcific AS • At least mild AR in 75% of patients
AR – Valvular disease II • Infective endocarditis • Leaflet perforation • Vegetation interferes with coaptation • Trauma • Bicuspid Valve • Can isolated regurgitation or stenosis, or both • Complication of catheter based ablation
AR – Valvular disease III • Myxomatous degeneration • Structural deterioration of bioprosthesis • Less common causes: • SLE, RA • Ankylosing spondylitis • Jaccoud arthropathy • Takayasu disease • Whipple’s disease • Anorectic drugs • Congential (rare, usually associated with bicuspid valve) • Membranous subaortic stenosis
Aortic root disease Dilation here is common; especially in AS; does not lead to AR • Between aorta proper and the annulus is a tube composed of collagen that forms sinuses of valsalva As little as 2mm of dilation here can cause AR Dilation here is rare
Aortic root disease • Dilation of the aortic ridge eliminates the normal overlap of the valves
AR – Aortic Root Disease • Age related (degenerative) • Systemic Hypertension • Aortic dissection • Cystic medial necrosis • either isolated or associated with Marphan syndrome • Bicuspid valve
AR – Aortic Root Disease II • Syphilitic aortitis • Osteogenesis imperfecta • Ankylosing spondylitis • Relapsing polychondritis • Ehlers-Danlos • Inflammatory bowel disease
AR – M-Mode • As the aortic jet cascades across the anterior MV leaflet it can create a high frequency fluttering • In acute AR premature closure of the MV can be seen • Due to rapidly increasing LV pressure
AR - M-mode • Fluttering of Anterior Mitral Valve leaflet • Increased duration between E and A peaks • Early example of using M-mode to indirectly assess valve disease
AR – 2D imaging • Detailed evaluation of valve and root • Detailed evaluation of LV size and function • Many important causes of AR easily seen on 2D evaluation • Even when AR is severe, sometimes 2D imaging is suprisingly normal
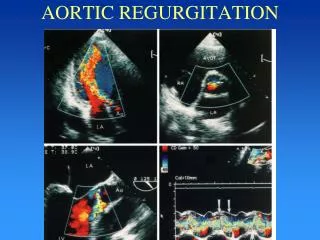
AR – Doppler Evaluation • Pulsed, continuous wave, and color flow Doppler are highly sensitive for detection of regurgitation and are complementary studies
Use of Doppler to Detect Regurgitant Jets • Most regurgitant jets >1.5 m/sec • CW lacks spatial resolution • PW needed to map location and direction of jet Mitral Inflow Identifies turbulence in an area; color flow derived from PW data Helpful for flow profile; gradient
AR – Pulsed Doppler • Early to assess severity of AR used pulsed Doppler to “map” AR • sample volume withdrawn towards apex to find length of regurgitant jet • Relies on turbulence during diastole on LV outflow side of AV • This assumes jet is centrally located and can be tracked towards apex • Another possible source of error:
AR MS
AR – Color Flow • Most common technique • Sensitivity >95% • False positive negatives; occur in tachycardia with mild AR • Frame rate allows only a few diastolic frames to be displayed • Can be overcome by using CW which has higher sampling rate • Specificity ~100%
AR – Color flow Doppler • Detects even trivial AR • 1% of subjects under 40 y.o. • 10-20% of patients greater than 60 y.o
Echo assessment: Vena Contracta • Measurement of the most narrow portion of jet behind the valve. • Mild: <3.0mm • Moderate: 3.0-5.9mm • Severe: >=6.0mm Enriquez-Sarano et al. Aortic Regurgitation. NEJM; 351:1539-46.
Echo assessment: Jet / LVOT height • Jet height to LVOT height ratio • Mild: 1-24% • Moderate: 25-46% • Moderate-severe: 47-64% • Severe: >=65% • Limitations: • Lateral resolution of color Doppler • Sensitive to angulation of ultrasound transducer Ekery, DL et al. Aortic Regurgitation: Quantitative Methods by Echocardiography. Echocardiography: 2000. 17; 294-302
AR – Continuous wave doppler • Because AR jet is high velocity, CW Doppler necessary to record envelope of jet. • The density of the jet compared with antegrade aortic flow is a (very simple) qualitative indication of the volume of regurgitation
AR – Continuous wave doppler AR Antegrade • Density is function of number of blood cells sampled and will generally increase with the regurgitant volume
AR – CW Doppler • Aortic regurgitant fraction can be estimated by ratio of reversed flow VTI / forward flow VTI in the distal aortic arch. Retrograde Antegrade Ekery, DL et al. Aortic Regurgitation: Quantitative Methods by Echocardiography. Echocardiography:2000. 17; 294-302
AR – Continuous wave doppler • Absolute gradient does not closely reflect amount of AR • Severity of AR can be described by the slope or the pressure half time • Pressure half time of less than 250 msec is an indicator of severe AR
AR - pressure half-time • Limitations: • Pressure half-time sensitive to chronicity of AR • acute AR leads to much shorter values than chronic AR when ventricle is dilated with increased compliance and can accommodate large regurgitant volumes. • Pressure half-time varies with systemic vascular resistance • vasodilators may shorten the pressure half-time even as the aortic regurgitant fraction improves.
AR - Regurgitant Volume or Fraction • Compare flow through aortic valve versus mitral or pulmonary valve. • Regurgitant volume (fraction): • Mild: <30cc (<30%) • Mild to moderate: 30-44cc (30-39%) • Moderately severe: 45-59cc (40-49) • Severe: >=60cc (>=50%)
AR - Regurgitant Volume or Fraction • Limitations: • Assumes normal flow through comparison valve. • Cannot be used in presence of shunts. • Sensitive to small measurement errors.
AR - Proximal isovelocity surface area • The PISA method can estimate regurgitant flow rate, and subsequently regurgitant orifice area).
AR - Proximal isovelocity surface area • Limitations of PISA • Isovelocity contour flattens as it approaches the orifice, underestimating flow. • Proximal structures can distort the isovelocity contour. • Sensitive to errors in radius measurement • 10% error in radius leads to 21% error in flow
Severe AR - Surgical Indications • Symptomatic patients (dyspnea or angina) • Normal, mildly depressed or moderately depressed LV • Surgery. • Severely depressed or dilated LV (EF<25% or LVESD>60mm) • High surgical risk (~10% operative mortality) but also poor outcomes with medical therapy.
Asymptomatic Severe AR - Surgical Indications • Preserved LV • Observe with serial echocardiograms. • Abnormal LV • “Rule of 55”: Surgery if: • LVEF <55% (ACC/AHA guidelines <50%) • LVESD > 55mm (or > 25 mm/m2). • Also surgery if LVEDD >70-75 mm • Uncertainty on which combination of criteria most useful.