Download
1 / 43
560 likes | 1.6k Views
Aortic Regurgitation and Aortic Leaflet Repair. Cesare Quarto MD. Clinical Scenario. A 48-year-old woman presenting with mild fatigue but no other symptoms, found to have a 3/6 diastolic cardiac murmur. BP 160/60 mm Hg; bounding peripheral pulses

E N D
Aortic Regurgitation and Aortic Leaflet Repair Cesare Quarto MD
Clinical Scenario • A 48-year-old woman presenting with mild fatigue but no other symptoms, found to have a 3/6 diastolic cardiac murmur. • BP 160/60 mm Hg; bounding peripheral pulses • Auscultation: decreased S1 and increased S2 intensity • TTE: bicuspid aortic valve with an eccentric jet of severe aortic regurgitation • LVEDD - 66 mm or 39 mmM2 of BSA • LVESD - 46 mm or 27 mmM2 of BSA • Ejection fraction - 51% How should this patient be treated?
Causeof AR • Developing Countries: rheumatic disease • Western Countries • In rare cases, aortic regurgitation is acute (Endocarditis, Aortic Dissection, Trauma) Congenital (Bicuspid Valve) Degenerative (annulo-ectasia)
Aortic Regurgitation Prevalence of AR is 4-7% of the population prevalence with age Severe regurgitation observed in men than women ( Framingham Heart Study)
Pathophysiology Increase in EDV and EDP Total SV= Regurg. Vol + forward SV LV volume overload ( indicated by enlarged LV on ECHO ) LV pressure overload ( indicated by increase end-systolic pressure ) BUT Symptoms develop slowlybecauseLeft atrial pressure increase late in the course of the disease
Symptoms Left sided heart failure: Dyspnoea, orthopnoea, fatigue, paroxysmal nocturnal dyspnoea Syncope and Angina due to reduced aortic diastolic BP Occasionally carotid artery pain
Signs Hyperdynamic circulatory state accounts the clinical signs of AR: • Hyperkinetic apical impulse • Increased systolic pressure and decreased diastolic pressure • Bounding pulses • Widened pulse pressure Loud early diastolic murmur Austin Flint murmur – MDM, maybe heard in severe AR, due to premature closure of MV by regurgitant jet and from the rapid increase in left ventricular diastolic pressure and making MV physiologically stenotic
Natural History Pts with Acute AR have poor prognosis without intervention Pts with Severe chronic AR in NYHA class III IV have an annual mortality of 25% Pts with Severe chronic AR in NYHA class II have an annual mortality of 6.3% N Engl J Med 2004;351:1539-46. Aortic Regurgitation,Maurice Enriquez-Sarano et All.
Natural History Pts asymptomatic with marked LV enlargment are associated with an increase risk (2%) of sudden death compared with the general population Pts asymptomatic without LV dysfunction do not have any excess risk of deathas compared with the general population, but do have high cardiovascular event rates (i.e., heart failure, or new symptoms) at 5 to 6 % per year N Engl J Med 2004;351:1539-46. Aortic Regurgitation,Maurice Enriquez-Sarano et All.
Diagnosis • Clinical examination • ECHO = Gold Standard • TOE • CMR • Angiogram • Exercise Testing
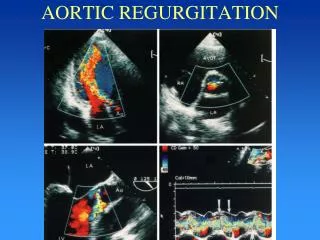
Echo assessment of AR • Anatomy: Diameter of annulus, S of Valsalva , STJ, AA, Aneurysm, Bicuspidy, LV diameter… • Mechanism: Dissection, Aneurysm of Aortic root, Leaflet prolapse, Endocarditis, Degenerative
Echo assessment of AR + Holodiastolic reversal flow in the descending aorta (= abdominal aorta).
Surgical options • Aortic valve replacement Mechanical Bioprosthetic/Biological (Stentles – Stented) Bovine Xenograft Allograft Homograft Porcine Equine Ross Cryo Homovital Problem with younger adult pts associated to anticoagulation and/or prosthesis durability
Surgical options • Aortic Valve repair If durable has the potential to be a good solution in younger adult pts
Clinical anatomy of the aortic root The aortic root is positioned to the right and postirior relative to the subpulmonary infundibulum
Clinical anatomy of the aortic root Forming the outflow tract from the LV and its function is supporting structure for the Aortic Valve, delineated superioly by the STJ and inferiorly by the VAJ Devided in : Structures distal to the attachments of the valvar leaflets ( Valvar Sinus) Structures proximal to the attachments of the valvar leaflets ( interleaflet or fibrous triangles)
Clinical anatomy of the aortic root The aortic root has been opened through a longitudinal incision across the area of aortic-mitral valvar continuity, and spread open to show the semilunar attachments of the valvar leaflets. Note the interleaflet triangles extending to the sinutubular junction, and the crescents of myocardium at the base of the two coronary aortic sinuses.
Clinical anatomy of the aortic root The valve leaflets are inserted into the aortic wall in a semilunar Fashion and their closure determined the valve competence in the central coaptation area; the level of the coaptation is at the middle distance between the nadir of their insertion and the commissural areas
Aortic Valve Repair Techniques of aortic valve repair have been documented for over 40 years. Starr and associates first reported a technique for aortic repair in 1960 [1] This was followed by two case reports of aortic valve repair by Spencer in 1962 and later Trusler in 1973 [2,3] In the early 1980’s, as percutaneous balloon valvotomy was performed [1] Starr A, Menashe V, Dotter D. Surgical correction of aortic insufficiency associated with ventricular septal defect. Surg Gynecol Obstet 1960;111:71– [2] Spencer FC, Bahnson HT, Neill CA. The treatment of aortic regurgitation associated with a ventricular septal defect. J Thorac Cardiovasc Surg 1962;43:222–33 . [3] Trusler GA, Moes CAF, Kidd BSL. Repair of ventricular septal defect with aortic insufficiency. J Thorac Cardiovasc Surg 1973;66: 394–403.
The functional classification of aortic root abnormalitiesresponsible for aortic insufficiency Functional classification of aortic root/valve abnormalities and their correlation with etiologies and surgical procedures El Khoury et All Curr Opin Cardiol. 2005 Mar;20(2):115-21. Department of Cardiovascular and Thoracic Surgery, Cliniques Universitaires Saint-Luc, Brussels, Belgium.
The functional classification of aortic root abnormalitiesresponsible for aortic insufficiency The aim of this classification is to provide a simple guide in the diagnosis of major abnormalities so that corrective surgical techniques can then be applied to each identified abnormality
Surgical procedures Type Ia: distal ascending aorta dilation, (STJ dilation) Type Ia lesions are treated by reduction of the circumference of the Sino-tubular junction and is usually achieved by replacing the ascending aorta with an appropriately sized Dacron graft. Ideally, its diameter should be approximately the size of the native aortic annulus
Surgical procedures Type Ib: proximal (valsalva sinuses) dilation and STJ dilation Remodeling of the aortic root Reimplantation of the aortic valve with creation of neo-aortic sinuses Type Ib lesions are treated by an aortic valve sparing operation, the remodeling technique (Yacoub) and the reimplantation technique (David operation)
Surgical procedures Type Ic: isolated FAA dilation CommissuralAnnuloplasty Circular Annuloplasty For the Type Ic the most appropriate surgical procedure may be a partial sub-commissural annuloplasty or circular annuloplasty
Surgical procedures Type Id: cusp perforation and FAA dilation Type Id lesions are treated by patch closure. For large defects autologous tricuspid leaflet tissue is used rather than autologous pericardium in the hope that will remain free from calcification
Surgical procedures Type II Cusp prolapse: leaflet plication (PL) LP repair with central plication. The normal free margin taken as reference Plication is extended with a short running suture, perpendicular to the free margin, 4—5 mm through the body of the leaflet in order to decrease leaflet distension
Surgical procedures Type II Cusp prolapse Gore-Tex resuspension (GTx) Resuspension with running suture of Gore- Tex 7/0. The 7/0 Gore-Tex suture is passed twice in the top of the commissure. Successively, two running sutures are passed over and over around the length of the free margin With gentle traction on each branch of the Gore-Tex sutures and applying opposite resistance with a forceps the free margin is shortened by slightly wrinkling the tissue
Surgical procedures Type II Cusp prolapse:The triangular resection The triangular resection involves excising a triangle of tissue in the middle of the prolapsing valve and then suturing the edges back together. A continuous suture is recommended instead of interrupted sutures because it decreases the chance of a leak and lessens thrombogenicity
Surgical procedures Type III Restrictive Cuspid motion Shaving, decalcification and valve extension with Three strips of pericardium, 3–8 mm that are sewn to the free edges of the valve cusps to extend them and increase the surface area for coaptation
Results: The Brussels Experience El Khoury et All Curr Opin Cardiol. 2005 Mar;20(2):115-21.
Results: The Brussels Experience El Khoury et All Curr Opin Cardiol. 2005 Mar;20(2):115-21.
Results: The Brussels Experience Actuarial survival curves. (a) Freedom from AR grade >2 in subgroups of patients having leaflet plication (PL), Gore-Tex resuspension (GTx) or the combination of PL + GTx and (b) freedom from AR grade >2 in subgroups of patients having triangular resection (TR) or pericardial patch repair (PP) alone or in combination with GTx
Result AV Sparing with AV Repair N =146 pts (a) Actuarial survival curve. (b) curve for freedom from recurrence of aortic regurgitation exceeding grade 2 or stenosis (including early and late recurrences) Gebrin El Khoury et All Ann Thorac Surg 2007;83:S746 –51
Results Aortic valve repair for aortic insufficiency in adults: a contemporary review and comparison with replacement techniques John Alfred Carra, Edward B. Savagea,b,*European Journal of Cardio-thoracic Surgery 25 (2004) 6–15
Discussion The optimal treatment of aortic insufficiency would be to replace or repair the valve to its pre-disease state, without the need for long-term anticoagulation and obtain life-long durability. Currently, no such treatment exists.
Discussion The risk of thromboembolism and infectious endocarditis is roughly equivalent The durability for valve repair seem less favorable than bioprosthetic replacement. ( difficoult comparison, Biopro mean age 72, repair mean age 36 ) Early durability of aortic valve repair is similar to that of pulmonary autograft, or homograft replacement valve in younger people, but later durability is worse
Conclusion • Repair may not be justified in older patients with excellent proven longevity of bioprostheses. • Bicuspid valves may be less amenable to reparative techniques than tricuspid valves, because the calcification in the bicuspid valve is more diffuse from free margin to aortic wall • Patients with rheumatic valvular disease appear to have an increased incidence of recurrence and repair failure.
Conclusion • Valve repair may be an option in carefully selected patients, in particular in association with procedure like valve-sparing • Valve repair is an established part of the treatment armamentarium for aortic valvular disease but is a technique in evolution, requiring better definition of successful approaches.